Download
1 / 44
440 likes | 457 Views
Explore the anatomy and functions of the excretory system, including kidneys, bladder, and ureters. Learn about urine formation, micturition reflex, and renal circulation. Understand the processes of filtration, reabsorption, and secretion.

E N D
Excretory System Tony Serino, Ph.D. Clinical Anatomy
Renal: Topic Objectives • Be able to describe and identify bladder and urethra anatomy and function, including differences between male and female. • Be able to describe micturition reflex. • Be able to describe and identify kidney anatomy, histology and function. • Be able to describe and identify circulation pattern to, from and within the kidney. • Be able to identify parts of the nephron and their functions. • Be able to describe urine formation and predict changes to output with changes in BP, ion pumps, and hydration status. • Be able to describe kidney contribution to acid/base balance and be able to predict kidney response to blood pH changes • Be able to describe hormonal BP control and predict response to low and high BP
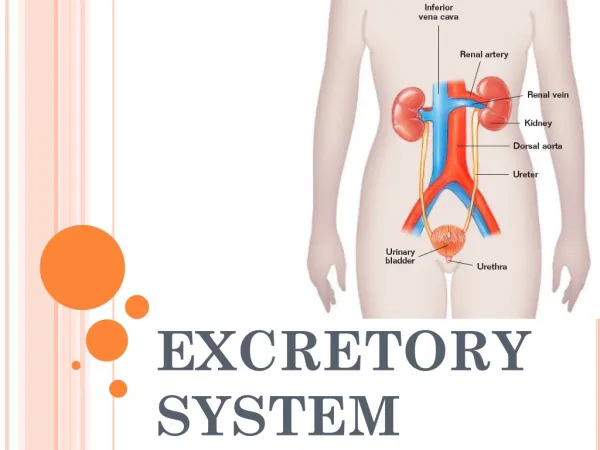
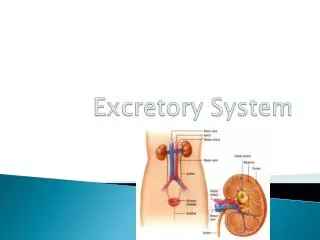
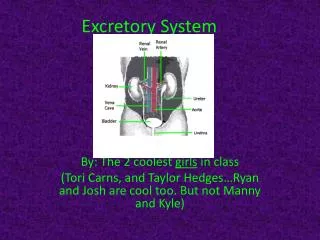
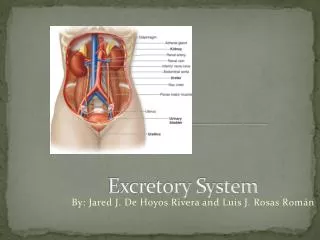
Excretory System • Remove wastes from internal environment • Wastes: water, heat, salts, urea, etc. • Excretory organs include: Lungs, Skin, Liver, GI tract, and Kidneys • Urinary system account for bulk of excretion
Ureter Histolgy -about 25 cm long, retroperitoneal, moves urine by peristalsis; volume of urine moved is called a jet (1-5 jets/min)-ureters enter the bladder wall obliquely, allowing them to remain closed except during peristalsis Adventitia Mucosa Muscularis
Urinary Bladder (Remanent of Allantois)
Urinary Bladder Histology Mucosa Submucosa Muscularis (Detrusor Muscle) (Serosa)
Urinary Bladder Filling • Highly distensible • 10-600ml normally • Capable of 2-3X that volume • Under normal conditions, the pressure does not significantly increase until at least 300 ml volume is reached
Urethra Histology -epithelium changes from transitional to stratified squamous along its length-large numbers of mucous glands present
Bladder (Storage) Reflex • As urine accumulates, the bladder wall thins and rugae disappear • Innervation (sympathetic) to the sphincter muscles (particularly the internal sphincter) keeps the bladder closed and depresses bladder contraction Voluntary control
Micturition Reflex (Voiding) • Urine volume increases, and the smooth muscle increases pressure in bladder • Stretch receptors in detrusor muscle, increase parasympathetic activity in the splanchnic nerve cause increase bladder contraction and internal sphincter relaxation • Voluntary relaxation of external sphincter by a decrease in firing of the pudendal nerve
Kidney Location (x.s.) (Retroperitoneal)
Cortex vs. Medulla Capsule
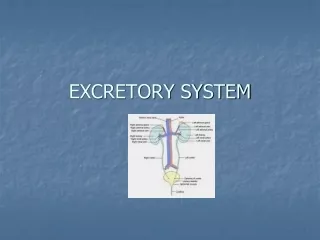
d Urine Formation Overveiw • Pressure Filtration • Reabsorption • Secretion • Reabsorption of water
Glomerulus Bowman’s Capsule
Filtration in Glomerulus Endothelium Capillary Lumen Basement Mem. Pedicels Slit pores Glomerular Filtrate Fenestration
Glomerular Filtration • A pressure filtration produced by the BP, fenestrated capillaries of glomerulus, and the podocytes creates the glomerular filtrate • Slit size allows filtration of any substance smaller than a protein • Blood proteins create an osmotic gradient to prevent complete loss of water in blood, • Pressure in Bowman’s capsule also works against filtration • Volume of filtrate produced per minute is the Glomerular Filtration Rate (GFR) • Average GFR = 120-125 ml/min
Tubular Reabsorption • 75-85% of glomerular filtrate reabsorbed in PCT • Some of the reabsorption is by passive diffusion • Example: Na+ • Much of the reabsorption is active, most linked to the transport of Na+; known as co-transport • The amount of transporter proteins is limited; so most actively transported substances have a maximum tubular transport rate (Tm)
Loop of Henle and CD • Provides mechanism where water can be conserved; capable of producing a low volume, concentrated urine • Loop of Henle acts as a counter-current multiplier to maintain a high salt concentration in medulla • CD has variable water permeability and must pass through the medulla • Allows for the passive absorption of water
Counter-current Multiplier • Descending is permeable to water but not salt; loss of water concentrates urine in tube • Ascending is permeable to NaCl but not water; Salt now higher in tube than interstitium; first passively diffuses out then near top is actively transported out • Results in a self-perpetuating mechanism; maintaining a high salt concentration in center of kidney
Vasa Recta • Supply long loops of Henle • Provide mechanism to prevent accumulation of water in interstitial space • Passive diffusion allows the blood to equilibrate with osmotic gradient in extracellular space
Tubular Secretion • PCT and DCT both actively involved in secretion (active transport of substances from the blood to the urine) • Both ducts play important roles in controlling amount of H+/HCO3- lost in urine and therefore blood pH • DCT actively controls Na+ reabsorption upon stimulation by aldosterone (controls final 2% of Na+ in urine)
Summary Re-absorption Water Re-absorptionwith ADH present Loses water Selective Secretion & Re-absorption Loses NaCl
Thirst Hypertonic, low volume urine Reabsorption of Water in CD ADH release
Renin-Angiotensin-Aldosterone iBP Decreased Stretch in JG cells Decreased Na in Urine in DCT h stimulation of Macula Densa h Renin Release Angiotensinogen g Angiotensin I h arteriolar constriction h BP Converting Enzyme Angiotensin II h Aldosterone Release h Na+ reabsorption h water retention and BV
Declining BP Regulation Stimulates thirst