Download
1 / 85
850 likes | 1.1k Views
Coronary Heart Disease Medication. Robert Hallworth Chair – Greater Manchester Non-Medical Prescribing Network. Oldham Primary Care Trust. CHD - so who do we mean and what should we look at?. Established - post MI, CABG, ischaemic stroke / TIA, angina, AF, PVD

E N D
Coronary Heart Disease Medication Robert Hallworth Chair – Greater Manchester Non-Medical Prescribing Network Oldham Primary Care Trust
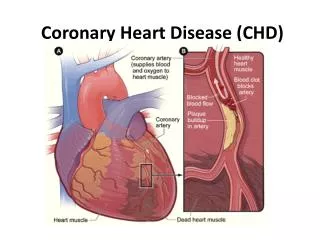
CHD - so who do we mean and what should we look at? • Established - post MI, CABG, ischaemic stroke / TIA, angina, AF, PVD • Heart failure • Hypertension • (Diabetes) • Raised cholesterol, obesity, smokers • Intervention + review based on current status, risk factors, existing treatment • Targets in the GMS contract
CaseIt is a busy day in your practice and you are sitting at your desk, legs up, leafing through a recent issue of Diversion, The Magazine for Physicians at Leisure. You come across an ad for Plavix,TM which states that this medication reduces the risk of cardiovascular events by 9% compared to aspirin. You wonder if you should be switching all your patients to Plavix. TM
Primary prevention:statin therapy [NICE 2008] • Offer statin therapy for adults who have a 20% or greater 10-year risk of developing CVD • Initiate treatment with simvastatin 40 mg • If simvastatin 40 mg is contraindicated, offer a lower dose or alternative preparation (such as pravastatin) • A target for total or LDL cholesterol is not recommended
Secondary prevention: statin therapy [NICE 2008] • Offer statin therapy to adults with clinical evidence of CVD • Offer higher intensity statin to people with acute coronary syndrome, taking into account: • the patient’s informed preference • comorbidities • multiple drug therapy, and • the benefits and risks of treatment
Secondary prevention: statin therapy continued • Treatment should be initiated with simvastatin 40 mg • If simvastatin 40 mg is contraindicated, offer a lower dose or alternative preparation (such as pravastatin) • If total cholesterol of < 4 mmol/litre or LDL cholesterol of < 2 mmol/litre is not attained consider simvastatin 80 mg (or similar)
Targets for PCT Advisers • Better Care Better Value • Statins • Generic Prescribing • National Audit Office • Proton Pump Inhibitors • ACE inhibitors / Angiotensin 2 Receptor Antagonists • Antiplatelets • Other important cost areas • Drugs used in diabetes • Respiratory corticosteroids • Analgesics • Hypertension and Heart Failure
What is our approach for primary and secondary prevention? Will this differ based on the age of our patient? Will this differ if our patient has diabetes?
A recent meta-analysisCholesterol Treatment Trialists' (CTT) CollaboratorsLancet 2005; 366: 1267-1278. • Statin therapy reduces the relative risk of major events by one fifth (20%) for every 1mmol/L reduction in LDL cholesterol (but is there really a linear relationship?). • This is largely irrespective of the initial lipid profile or other presenting characteristics. • The absolute benefit relates chiefly to an individual's absolute risk of such events and to the absolute reduction in LDL cholesterol achieved. • Statins at established doses (e.g. simvastatin 40mg) can reduce LDL cholesterol by at least 1·5mmol/L in many patients, and hence would be expected to reduce the incidence of major vascular events by about one third. • The possibility that higher doses would result in clinically relevant adverse effects cannot be excluded.
Summary of High-Dose POO Studies • A-Z study(JAMA 2004; 292: 1307-1316) – simvastatin 80mg vs. no statin/20mg simvastatin after AMI: No significant benefit, problem with harms on higher dose – myopathy and rhabdomyolysis • PROVE-IT(N Engl J Med 2004; 350: 1495-1504) – atorvastatin 80mg vs. pravastatin 40mg post ACS: Significant benefit not much harm seen • TNT(N Engl J Med 2005; 352: 1425-1435) – atorvastatin 80mg vs. atorvastatin 10mg in stable CHD (but who responded well to atorvastatin in the “run-in”): Significant benefit but also significant harm • IDEAL(JAMA 2005; 294: 2437-2445) – atorvastin 80mg vs. simvastatin 20mg in stable CHD:No significant benefit, some harm • SPARCL(N Engl J Med 2006; 355: 549-559) – atorvastatin 80mg vs. placebo in stroke/TIA:Significant benefit, some harm
Use a statin in patients with ACS de Lemos JA, et al. JAMA2004; 292: 130716 Cannon CP, et al. N Engl J Med 2004; 350: 1495504 Pedersen TR, et al. JAMA 2005; 294: 243745 • Phase Z of the A to Z trial showed no difference in event rates between simvastatin 40mg od for 1 month followed by 80mg od compared to placebo for 4 months followed by simvastatin 20mg od. There were 3 cases of rhabdomyolysis in patients receiving 80mg simvastatin. • PROVE-IT compared pravastatin 40mg to atorvastatin 80mg. The primary endpoint was time to first of death, MI, re-hospitalisation for UA, revascularisation or stroke. 22.4% of patients in the atorvastatin arm had these events at 2 years compared to 26.3% in the pravastatin group. • IDEAL showed no difference in the primary endpoint of time to first coronary death, MI or resuscitated cardiac arrest between simvastatin or atorvastatin
Statins • Baseline • Serum cholesterol, LFTs, CK, U&Es (rosuvastatin), TFT • Routine • Cholesterol • Every 12 months • CK • Within 1-3 months & when cholesterol checked, after dose increase or when given with a fibrate • LFTs • Within 1-3 months, then at 6 and 12 months or if hepatotoxicity suspected (greater risk with higher doses – rosuvastatin 40mg / simvastatin 80mg)
Discontinuing statins • Serum transaminases at 3 x upper limit of normal • Beware higher doses • If myopathy occurs (daily discomfort) • CK > 5 x upper limit of normal • Liver disease is likely to be obstructive
Cholesterol measurements in the first few years of statin treatment may mislead • Galsziou P et al. Monitoring cholesterol levels: measurement error or true change? Ann Intern Med 2008; 148: 656-61 • Health professionals should be wary of increasing a patient’s lipid-lowering treatment on the basis of a single cholesterol test if they are reasonably confident that the patient is taking the medication as prescribed.
OTC Simvastatin • Is an initial cholesterol test needed? • How often do LFTs and CK need monitoring? HPS suggests: Up to 40mg simvastatin adverse effects = placebo
SEAS and ezetimibe: no benefits on CV endpoints, questions raised over cancer risk • Rossebo AB et al for the SEAS Investigators. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med 2008; 359 • It would seem sensible to use ezetimibe only with caution as there is no published evidence of its benefit on clinically important outcomes such as cardiovascular events and its long-term safety is unknown
Fibrates • Baseline – serum cholesterol, LFTs, CK • Routine – cholesterol (every 12 months), LFTs (every 3 months for 1 year), FBC (gemfibrozil every 3 months for 1 year) • DISCONTINUE: • Serum transaminase ≥ 3 x ULN • Myopathy symptoms or CK > 10 x ULN
Omacor • Licensed for hypertriglyceridaemia (high dose) and secondary prevention of MI (low dose). • Main data comes from Gissi-Prevenzione trial • Is this representative of UK patients?
NICE CG 54 - Hypertension • Offer drug therapy to patients with: • persistent high blood pressure of 160/100 mmHg or more • persistent blood pressure above 140/90 mmHg and raised cardiovascular risk (10-year risk of cardiovascular disease of at least 20%, existing cardiovascular disease or target organ damage). • Aim to reduce blood pressure to 140/90 mmHg or less, adding more drugs as needed, until further treatment is inappropriate or declined.
ALLHAT (JAMA 2002) • “The key message from ALLHAT is that what matters most is getting blood pressure controlled, and that this is overwhelmingly more important than the means. Combinations of several drugs will be required for most patients, and such an antihypertensive treatment cocktail should include a thiazide diuretic”
The Moral of the Tale • As long as we reach the objective (130/80), it doesn’t matter how we get there
Comparing Interventions(Clinical Evidence) • Primary prevention, to prevent CHD / CHD death: • Tight BP control NNT 14 • Tight BG control NNT 46 • Tight BG control, metformin NNT 16 • Statin NNT 27 • Aspirin NNT 16-39 • Ramipril NNT 22
Hypertension in Diabetes [NICE 2008] • First choice antihypertensive drug is a once-daily ACE inhibitor • (Plus a diuretic and / or calcium channel blocker in people whose blood pressure is not controlled to target on monotherapy) • A calcium channel blocker is recommended for women who may become pregnant
ARBs as effective as ACE inhibitors in CV risk reduction? – Jury still out • The TRANSCEND study reinforces the importance of only prescribing ARBs as an alternative to ACE inhibitors where there is clear intolerance to ACE inhibitors. • Lancet 2008; 372: 1172-83.
Angina - Treatment Options • Immediate relief of symptoms • GTN • Long-term prevention of symptoms • Beta-blocker • Calcium channel blocker • Nitrate • Potassium channel activator
Combination therapy • With a maximal dose beta-blocker add • Long acting dihydropyridine • ISMN or nicorandil • If a beta-blocker is contra-indicated use: • CCB – add ISMN or nicorandil • Nitrate – add CCB or nicorandil • There is no evidence that a third drug improves symptom control
Adverse Effects • Antiplatelets • Beta-blockers • Calcium-channel blockers • Nitrates • Nicorandil
Myocardial Infarction [NICE CG43 May 2007] • Give low dose aspirin (75mg daily) – clopidogrel if allergy (NSTEMI / STEMI) • Give beta-blockers – ALL patients EARLY for at least 2-3 years • Give ACE inhibitors – ALL patients EARLY • Provide advice and treatment to control BP • Give statins of low acquisition cost ASAP to reduce cholesterol to target • Tackle other risks such as blood glucose levels, smoking, physical activity, diet and weight
Relative Risk(RR) = Risk (Rx)/ Risk (Pl) = .08/.12 = .67 Relative Risk Reduction (RRR) = 1 - RR = 1- .67 = .33 or 33%
Absolute Risk Reduction (ARR) = Risk (Pl) - Risk (Rx) = .12 - .08 = .04 or 4%
Number Needed to Treat (NNT):NNT = 1/ARR Number of patients needed to treat to prevent one outcome
NNT = 1/ARR ARR = 4%NNT = 1/.04 = 25
Check-list • Are the risks relative or absolute?
Check-list • Are the risks relative or absolute? Relative. Absolute = 0.9%
Check-list • Are the risks relative or absolute? Relative • Is the result statistically significant?
Check-list • Are the risks relative or absolute? • Is the result statistically significant? Yes, marginally. P = .045 95% CI (0.3% to 16.5%)
Check-list • Are the risks relative or absolute? Relative • Is the result statistically significant? Yes • Is the result clinically significant?
Check-list • Are the risks relative or absolute? Relative • Is the result statistically significant? Yes • Is the result clinically significant? No NNT = 1/ARR =1/.009 =111 95%CI (57 - 2500)