Download
1 / 29
290 likes | 624 Views
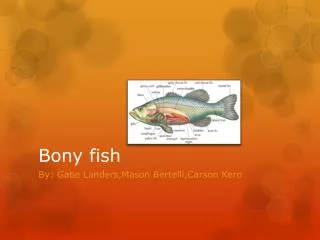
Bony Thorax. Spokane Community College Radiology Film Critique. 1. Manubrium. 2. 3. 4. Body. 5. Xiphoid. 6. 7. 8. 9. 10. 11. 12. RIBS. Routine views : AP above AP below RPO of the affected side LPO of the affected side. Structures shown:.

E N D
BonyThorax Spokane Community College Radiology Film Critique
1 Manubrium 2 3 4 Body 5 Xiphoid 6 7 8 9 10 11 12
RIBS • Routine views : • AP above • AP below • RPO of the affected side • LPO of the affected side
Structures shown: • AP projection shows the posterior ribs, above or below the diaphragm
Good film • For ribs above the diaphragm, posterior ribs 1-10 from both sides should be seen above the diaphragm and include in their entirety • For ribs below the diaphragm, posterior ribs 8-12 from both sides should be seen below the diaphragm and include in their entirety • Ribs should be seen clearly through the lungs or abdomen according to the region examined
Structures Shown: • RPO/LPO in this projection the axillary portion of the ribs are projected free of self-superimposition LPO Left side down
Grashey Scap “Y” RPO Upper Ribs Right side down
RPO Lower Ribs
Good film: • There should be approximately twice as much distance between the vertebral column and the outer border of the ribs on the affected side as there is on the unaffected side • Axillary portion of the ribs should be demonstrated free of superimposition
Sternum • Routine views: • RAO • Lateral
What is shown: • This method shows a slightly oblique PA projection of the sternum. The breathing motion obliterates the pulmonary markings • Structure shown: The entire sternum from jugular notch to tip of xiphoid
Good Film: • Entire manubrium to the tip of the xiphoid should be included • Visibility of the sternum through the thorax should be reasonably good • Sternum should be projected just free of superimposition from vertebral column • Sternum should be projected into the cardiac shadow • **Breathing technique: to blur pulmonary markings
Structureshown: • Lateral projection of the entire length of the sternum is demonstrated showing the superimposed sternoclavicular joints and medial ends of the clavicles
Sternoclavicular Articulations: • RAO • LAO • Axiolateral-Kurzbauer method of the affected side (not in book)
Structures shown: • This method presents a slightly oblique projection of the sternoclavicular joints. Shows the joint closer to the film with less distortion. **LAO: Left side down: The joint closest to the IR is shown (left)
LEFT LAO
Good film: • SC jnts of interest should be in the center of the film (down side) • Manubrium and medial ends of clavicles should be included • SC jnts space should be open • SC jnts of interest should be directly in front of the vertebral column with minimal obliquity • Visibility of the SC jnt through the superimposing rib and lung fields should be reasonably good
Adjust the position of the cassette so that its midpoint will coincide with the CR. Respiration is suspended at the end of full inhalation. Direct the CR through the lowermost sternoclavicular articulation at an angle of 15 degrees caudal.
Structures shown: This method presents an unobstructed lateral projection of the sternoclavicular articulation adjacent to the film
Good film: • SC jnt of interest should be demonstrated • Shoulders should not superimpose the SC articulations.