Download

1 / 43
430 likes | 703 Views
FY 2012 Hospital Rate Setting. Wisconsin Department of Health Services Division of Health Care Access and Accountability Bureau of Fiscal Management March 22, 2011. Agenda. Rate Setting Timeline Governor Walker’s 2011-2013 Budget Request FY 2011-2013 Hospital Budget Policy Issues

E N D
FY 2012 Hospital Rate Setting Wisconsin Department of Health Services Division of Health Care Access and Accountability Bureau of Fiscal Management March 22, 2011
Agenda Rate Setting Timeline Governor Walker’s 2011-2013 Budget Request FY 2011-2013 Hospital Budget Policy Issues FY 2011 Pay-For-Performance Measures for Acute Care, Children and Rehab Hospitals FY 2010 Hospital Assessment FY 2011 Hospital Assessment Next Meetings Agenda
FY 12 Rate Setting Timeline March 22nd – Kick Off Meeting • Overview of Governor Walker’s MA Budget Provisions April 20th • Present DRG Weights • Discuss Policy Decisions • Announce FY 2011 Pay-For-Performance Measures May 31st • Present State Plan • Present Draft Hospital Rates June 21st • Present Final Hospital Rates • Announce FY 2012-2013 Pay-For-Performance Earn-Back Measures July 1st – FY 12 Rates Effective
Medical Assistance 20011-13 Biennial Budget:Medical Assistance Program Parameters
Key Elements of Medicaid Programs Eligibility Eligibility requirements are based on income and age; certain programs having disability-related requirements. The American Recovery and Reinvestment Act of 2009 (ARRA) and the Patient Protection and Affordable Care Act of 2010 (ACA) impose requirements on the extent to which states can restrict eligibility standards. Medicaid programs have mandatory eligibility groups for whom the state must provide health care benefits and optional groups for whom the state may expand coverage. Benefits Eligibility determines the benefit plan of members, which in turn determines benefits received. Benefits are provided through a wide range of individual practitioners, hospitals, nursing homes, managed care organizations and local governmental entities such as county public health departments and school districts. Providers must be certified by the Medical Assistance Program. Payments State Medicaid rates and benefit plan utilization establish the maximum fee paid to providers for Medicaid covered benefits. The federal medical assistance percentage (FMAP) is the portion of the total payment for covered services supported by federal matching funds. Efficient Health Care Purchasing The department continually seeks to reduce MA costs for providing quality health care by promoting cost-effective services and maximizing the receipt of federal revenue. 5 5
Medical Assistance 20011-13 Biennial Budget:Enrollment & Expenditure Trends
ExpenditureHistory for Medical Assistance Over the past five years, expenditures for the Medicaid programs have increased an average of 11 percent per year, growing from $4.4 billion all funds in fiscal year 2006 to $6.6 billion in fiscal year 2010.
The economic recession that began in December 2007 caused a prolonged spike in MA enrollment for states across the country. The federal government relieved enrollment pressure by providing higher federal matching payments (FMAP) through the American Recovery and Reinvestment Act. The enhanced FMAP is scheduled to end July 1, 2011, leaving states to fund a greater share of persistently high enrollment.
Medical Assistance Shortfall Actions in Other States The scheduled reduction of FMAP payments to states has created fiscal problems nationally and forced states to contemplate severe reductions to medical assistance programs. • Arizona has proposed suspending Medicaid coverage for 280,000 people. • New York State is proposing a 2% across-the-board decrease in Medicaid funding. • Georgia has proposed dropping dental and vision coverage. • California has proposed cutting Medicaid by $1.7 billion, in part by reducing provider payments by 10%. • Maryland proposes cutting payments to hospitals by $264 million – on top of $133 million in hospital cuts over the past three years.
The Governor’s plan for Medicaid will reduce expenditures by $500 million in the next biennium compared to the pre-recession trend. For future years, those savings continue to grow, totaling $1.2 billion all funds by fiscal year 2017.
Governor Walker’s Medical Assistance20011-13 Biennial Budget Proposal
For Wisconsin, the FY 2011–2013 MA budget will need an additional $1.26 billion in GPR over the biennium just to replace lost federal funding. Combined with cost increases, the Medicaid budget would require an additional $1.8 billion in additional GPR over the biennium, representing 7% of estimated FY2011-13 general fund tax revenue.
Eligibility Reform versus Eligibility Limits The Patient Protection and Affordable Care Act (PPACA) allows for states experiencing a budget deficit to lower eligibility limits and drop coverage for any non-pregnant, non-disabled adults with family income above 133% FPL. This means that beginning on July 1, 2011 the federal government would allow Wisconsin to eliminate coverage for approximately 70,000 enrollees who meet these parameters -- the cost savings of dropping their coverage is estimated to be $57 million annually. PPACA does not allow Wisconsin to make other, less severe, changes to eligibility in order to avoid eliminating coverage for thousands of adults. If given the flexibility to adjust eligibility standards, Wisconsin could retain coverage for these adults. 14
Flexibility to Modify Eligibility Requirements (cont’d) • In lieu of eliminating coverage for many adults, DHS is preparing a package of reasonable, targeted eligibility changes to ensure that program resources are targeted to those most in need who have no other means to access health care. These include: • Reviewing the standards for state residence; • Revising retroactive eligibility and eligibility grace period policies; and • Enforcing current policies to improve the accuracy of eligibility determinations. 15
Flexibility to Modify Eligibility Requirements To achieve significant savings in the MA program, Wisconsin needs authority from the federal government to waive certain federal maintenance of effort (MOE) requirements contained in PPACA. PPACA essentially freezes state MA eligibility standards to what was in effect on March 23, 2010; thus, Wisconsin is prohibited from using many of the cost containment tools that would otherwise be available. DHS is seeking a waiver for the MOE restrictions from the federal government. If the federal waiver is not approved by January 1, 2012, DHS will be forced to eliminate coverage for non-pregnant, non-disabled adults within family incomes above 133% FPL as of July 1, 2012. 16
Modifying or Eliminating Optional Benefits There are mandatory and optional services that all states are required to or have the option to provide. Optional benefits include, but are not limited to: prescription drugs, vision services, dental services & dentures, clinic services, chiropractic services, therapies, durable medical equipment and supplies, respiratory care for vent-dependent members and community-based long-term care services such as personal care. States have the flexibility to ask the federal government to expand or reduce the optional benefits they provide, and some states are eliminating optional benefits in order to reduce their program costs. At this time, DHS is not pursuing the elimination of any optional services. 17
Reductions in Provider Reimbursement MA reimburses providers through rates set in the department’s maximum fee schedules depending on the services provided. A number of states have imposed either targeted rate cuts for specific provider types or broad across-the-board reduction applied to many if not all provider types. Another option is better alignment of Wisconsin’s rates to the rates paid through the federal Medicare program. 18
Realigning Provider Incentives to Achieve Better Outcomes The department will review reimbursement policies to better realign provider incentives with improving care outcomes. The goal of this effort will be to ensure the appropriate care is provided in the appropriate setting at the appropriate time. 19
Aligning Coverage with Other Private Payers’ Policies Reducing the Crowd-Out of Other Health Insurance: MA has traditionally been the payor of last resort. However, recent program expansions have loosened these requirements, allowing individuals to choose between coverage through MA over coverage available through other options. For BC+, this will mean that young adults eligible for coverage on their parents policies will need to sign up for that coverage. All Funds Savings Estimate: FY 12: $3.25 million FY 13: $3.26 million For SeniorCare, it will require seniors eligible for Medicare Part D to participate in that program in order to be eligible for SeniorCare. The Program will still be available to interested seniors and can provide wrap-around benefits to augment coverage available under their Part D plans. All Funds Savings Estimate: FY 12: $18.3 million FY 13: $36.6 million 20
Improving Care Coordination The department can achieve both fiscal savings and improved quality of care through the increased use of care coordination. The department will develop models of service delivery, including health homes, to more effectively manage the care of recipients. The department will also implement systems to coordinate care across Medicaid and Medicare for individuals eligible for both programs. 21
Changes in Family Care Enrollment Family Care began as a 5-county pilot program in 2000 that began to rapidly expand beginning in the 2007-09 biennium. At the end of the 2009-11 biennium, Family Care will be available in 57 of Wisconsin’s 72 counties, covering 79% of the state’s adult population. Amidst this broad expansion there has been no adequate review of the effectiveness of the program in meeting the care needs of the clients and providing services in a cost effective manner. The non-partisan Legislative Audit Bureau is now conducting just such a comprehensive review. Until that review is complete the department will defer all further expansion of the program. 22
Administration of Medical Assistance Determining eligibility and providing on-going case maintenance for Wisconsin’s income maintenance (IM) programs varies by county and eligibility group. Levels of performance and customer service vary from county to county. The Governor proposes consolidating these functions, creating a state-administered IM service delivery model, consolidating all administrative functions and using state-workers for oversight and public worker mandated functions. Goal is to make administration more cost effective and work with community partners for outreach and better customer service. These changes will improve the accuracy and timeliness of eligibility determinations, while reducing the total IM and decreasing the number of income maintenance staff. 23
Health Care Efficiency Measures DHS will need to implement a wide array of health care efficiency measures during the next biennium to contain costs while maintaining and improving quality. To identify and develop these efficiency measures, DHS will seek input from providers and advocates. These measures will include a review of everything from improving administrative processing procedures to the provision of medical services and ways to strengthen efforts to reduce recipient and provider fraud and abuse. 24
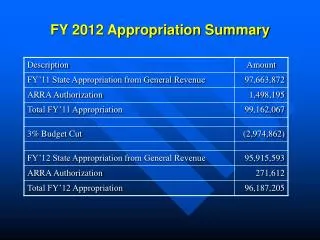
MA Biennial Base ReestimateGeneral Purpose Revenue Funding DHS September Request: $0.5 billion With Changes to Request: $1.8 billion Increased Caseload Decreased FMAP Assumption Froze Hospital Assessment Deleted Rate Reform 3.0 DOA Governor’s Request: $1.3 billion ` Eligibility and Efficiency Reforms and/or Reductions
Governor Walker’s 2011-2013 HospitalBudget Request *Final budget numbers will be based on the budget which is subject to legislative changes
Hospital Budget Components • Caseload Assumption • Intensity Assumption • Assessment Payments
Hospital Intensity Assumptions • The Governor’s Budget Request changed the Hospital Intensity from 2% to 0% with an additional 1% withheld. • The 1% withheld will be available for Hospitals to Earn-back by performing well on several Pay-for-Performance Measures.
Intensity Pay-For-Performance Earnback Provision Hospitals will be able to earn back 1% of the intensity 2012 and 2013. Source to Measure Data: FY 2009-2011 Medicaid Claims Data The department is currently reviewing the data and Medicare Performance Measures to determine which measures will be chosen. There may be different measures for different types of hospitals. Hospitals will be given a chance to review data for completeness.
Hospital P4P Earn-Back Provision Performance Data • Historical Medicaid Claims Data Possible Performance Measures • Hospital Readmissions within 30 Days • Appropriate ER Usage • Maternity Indicators (Discharge Follow-up) • Mental Health Indicators Hold-Back Amount • 1% of Hospital Rates will be available to win back under this provision.
Medicare Part A Cutback • The Governor’s Budget assumes the Medicaid Program will begin to cutback on Medicare Part A claims. • This proposal will limit what Medicaid pays Hospitals for Medicare Part A Coinsurance. • The All Funds cost savings in the Governor’s Budget Request :
Health Care Efficiency Measures DHS will need to implement a wide array of health care efficiency measures during the next biennium to contain costs while maintaining and improving quality. To identify and develop these efficiency measures, DHS will seek input from providers and advocates. These measures will include a review of everything from improving administrative processing procedures to the provision of medical services and ways to strengthen efforts to reduce recipient and provider fraud and abuse. 34
FY 2011-2013 Hospital Assessment Budget Assumptions • The Governor’s Budget Request holds the Hospital Assessment Amounts steady at the FY 2011 levels. • The tax percentage will likely decrease for FY 12 and FY 13.
FY 2012 Policy Issues • Modify Current Trim Points. • Review how budget is set for Critical Access Hospitals vs. Acute Care Hospitals. • Move to Ambulatory Payment Classification for Outpatient Rates starting 1/1/2012. • Pay Labs on Max Fee Schedule. • Other Ideas?
FY 2011 Pay-For-Performance Measures for Acute Care, Children’s and Rehab Hospitals • For FY 2011, $5,000,000 has been allocated for Pay-For-Performance Measures • Payment will be based on CheckPoint Data • DHS will work with WHA to determine appropriate measures. • The methodology will focus on Performance rather than Reporting.
FY 2010 Hospital Assessment • The department submitted the FY 2010 Hospital Assessment Report to the Legislature in January. • The department shut off access payments for 2010 claims on February 11, 2011. • Report is available as handout. • If you have any questions regarding the report, please contact Krista Willing by email at KristaE.Willing@wi.gov or (608) 266-2469.
FY 2011 Hospital Assessment • The department will provide a projection of the FY 2011 Hospital Assessment at the April Rate Setting Meeting. • At least partial HMO Payments will be made for both May and June this year.
Next Meeting Agenda • Present DRG Weights • Discuss Policy Decisions • Announce FY 2011 Pay-For-Performance Measures • FY 2011 Hospital Assessment Update April 20th 9:00am-12:00pm 1 West Wilson Street CR 751