Download
1 / 53
590 likes | 1.06k Views
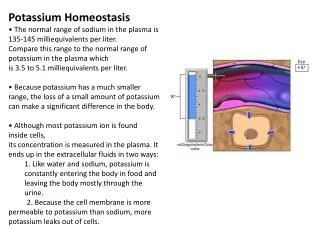
POTASSIUM BALANCE. Ronen L, MD NEPHROLOGY AND HYPERTENSION SERVICES HADASSAH UNIVERSITY HOSPITAL. Internal regulation. External regulation. Role of Insulin and β - adrenergics on the Distribution of K. Shift of K Out of cells in Metabolic Acidosis.

E N D
POTASSIUM BALANCE Ronen L, MD NEPHROLOGY AND HYPERTENSION SERVICES HADASSAH UNIVERSITY HOSPITAL
Internal regulation External regulation
Shift of K Out of cells in Metabolic Acidosis Monocarboxylic acids enter the cells in an electorneutral fashion. Therefore they do not cause a change in cell voltage. H load of inorganic acid is titrated by HCO3in the ECF→ ↓ cell voltage→ K shifts out of cell
Factors Affecting Potassium Secretion From the Tubular Cell to the Lumen • K+ concentration gradient across the luminal membrane • Electrical gradient across the tubular cell • K+ permeability of the luminal membrane
Effects of aldosterone actions in principal cells • Increases the permeability of the luminal membrane to Na by increasing the number of open ENaC→increases electrical gradient across the tubular cell • Increases the permeability of the luminal membrane to K by increasing the number of open K channels • Enhances the activity of the Na-K-ATPase at the basolateral membrane→increases cell K concentration
Regulation of Potassium Secretion-Serum Potassium Concentration • Direct effects: enhances Na+-K+-ATPase activity, increases luminal permeability to K+ and Na+. • Indirect effect: increases aldosterone secretion.
Regulation of Potassium Secretion- Distal Flow Rate • Increase in distal flow rate enhances K+ secretion. • It dilutes K+ secreted from the tubular cells to the lumen, and by doing so increases the K+ CONCENTRATION GRADIENT. • High flow rate also delivers more Na+ to the distal tubule, more Na+ is reabsorbed, and the gradient across the tubular cells rises, promoting K+ SECRETION.
RENAL RESPONSE TO POTASSIUM DEPLETION (LOW INTAKE OR NON RENAL LOSSES) K+ DEPLETION DECREASED ALDOSTERONE SECRETION DECREASED K+ IN TUBULAR CELLS INCREASED ACTIVITY OF H+-K+-ATPase DECREASED TUBULAR EXCRETION OF K+ INCREASED REABSORPTION OF K+ DECREASED URINARY EXCRETION OF K+
RENAL RESPONSE TO POTASSIUM LOADING K+ LOAD INCREASED ALDOSTERONE SECRETION DECREASED ACTIVITY OF H+-K+-ATPase INCREASED K+ IN TUBULAR CELLS AND PLASMA INCREASED TUBULAR EXCRETION OF K+ DECREASED REABSORPTION OF K+ INCREASED URINARY EXCRETION OF K+
HYPOKALEMIA • DECREASED NET INTAKE • INCREASED ENTRY INTO CELLS • INCREASED GASTROINTESTINAL LOSSES • INCREASED URINARY LOSSES • INCREASED SWEAT LOSSES • DIALYSIS • POTASSIUM DEPLETION WITHOUT HYPOKALEMIA
*usu. Decreased intake and volume depletion leading to increased aldosterone contribute Major causes of hypokalemia
Causes of Mineralocorticoid Excess • PRIMARY HYPERALDOSTRONISM A. Adenoma B. Hyperplasia C. Carcinoma • CUSHING DISEASE • LIDDLE’S SYNDROME • CHRONIC INGESTION OF EXOGENOUS MINERALOCORTICOID • HYPERRENINISM A. Renal artery stenosis B. Renin secreting tumor • HYPERSECRETION OF DEOXYCORTICOSTERONE OR OTHER MINERALOCORTICOID • LICORICE or CABENOXOLONE INGESTION- inhibits 11b-hydroxysteroid dehydrogenase which converts cortisol to cortisone • APPARENT MINERALOCORTICOID EXCESS
Liddle’s syndrome Autosomal dominant. Characterized by activating mutation in collecting duct Na+ channel with enhanced sodium reabsorption. Low renin, low aldosterone levels. The clinical picture mimics primary hyperaldosteronism: hypertension, hypokalemiaand alkalosis
Barrter’s and Gitelman’s syndromes • Impairment in one of the transporters involved in sodium chloride reabsorption in the loop of Henle (Bartter’s) and distal tubule (Gitelman’s) • The tubular defects in sodium chloride transport are almost identical to that seen with chronic ingestion of a loop diuretic (mimicking Bartter syndrome) or a thiazide diuretic (mimicking Gitelman syndrome). • Impaired sodium chloride reabsorption leads to mild volume depletion and activation of the renin-angiotensin-aldosterone system. • The combination of secondary hyperaldosteronism and increased distal flow and sodium delivery enhances potassium and hydrogen secretion at the secretory sites in the connecting tubules and collecting tubules, leading to hypokalemia and metabolic alkalosis
Barrter’s syndrome • Bartter syndrome is an autosomal recessive disorder that often presents in childhood and may be associated with the following clinical features: • Growth and mental retardation • Hypokalemia • Metabolic alkalosis • Polyuria and polydipsia due to decreased urinary concentrating ability • Normal to increased urinary calcium excretion • Normal or mildly decreased serum magnesium concentration
Gitelman’s syndrome • Gitelman syndrome is an autosomal recessive disorder that presents with hypokalemia, metabolic alkalosis, hypomagnesemia, hypocalciuria, and normal blood pressure • Manifestations include:: • Cramps of the arms and legs, due at least in part to hypokalemia and hypomagnesemia • Fatigue, which may be severe • polyuria and nocturia
proximal convuluted tubule Na HCO3 Collecting duct
Hypokalemia– Sympatology • Muscle weakness or paralysis • Cardiac arrhythmias • Rhabdomyolysis • Renal dysFx • Impaired concentration ability • Increased ammonia production • Impaired urinary acidification • Increased bicarbonate reabsorption • Renal insufficiency
Hypokalemia– ECG • ST depression • Decreases amplitude of T wave • Increased amplitude of U wave • Prolongation of PR interval • Widening of the QRS complex
Hypokalemia- diagnosis • ANAMNESIS • PHYSICAL EXAMINATION • URINARY K+ EXCRETION • ACID BASE STATUS
Hypokalemia– Treatment • KCl: the most common supplement • ADVANTAGES: • correction of alkalosis, • remains extracellular, and corrects membrane potential more effectively.
Hypokalemia– Treatment • KCL CAN BE GIVEN ORALY OR I.V. • ORALLY- CAN BE GIVEN IN LARGE DOSES BUT CAN CAUSE GASTRIC ULCERS. • I.V SHOULD BE GIVEN VERY SLOWLY UP TO 10-20 mEq/hr, AND AT LOW CONCENTRATION, UP TO 40-60 mEq/L.
Hypokalemia– Treatment • CONTINUE MONITORING K+ PLASMA LEVELS. • CONTINUE FOLLOWING CONTINUOUS LOSS OF K+
Hyperkalemia- Etiology • INCREASED INTAKE • EXIT OF K+ FORM CELLS TO EXTRACELLULAR FLUID • DECREASED URINARY EXCRETION
Hyperkalemia– Etiology: Increased Intake • Rare as a cause for hyperkalemia when renal K+ excretion is intact. • Acute K+ load, oral or IV. Can cause transient hyperkalemia.
Pseudohypoaldosteronism RESISTANCE TO ALDOSTERONE: HYPERKALEMIA, HYPOTENSION OR HYPERTENSION * ACQUIRED: mostly in tubulointerstitial diseases of the kidney. * CONGENITAL: RARE! 1. TYPE 1: salt wasting, hypotension and hyperkalemia, high levels of renin and aldosterone. Genetics: loss-of-function mutations in MR, or mutations in subunits ofENaC. 2. TYPE 2: Gordon’s syndrome: hypertension, hyperkalemia, metabolic acidosis. genetics: mutation in WNK4 or gain-of-function mutation in WNK1.
Hyperkalemia- symptoms • MUSCLE WEAKNESS • CARDIAC ARRHYTHMIAS
Hyperkalemia- ECG • PEAKED, NARROWED T WAVES • SHORT QT INTERVAL PRLONGATION OF PR INTERVAL • WIDENING OF QRS COMPLEX • LOSS OF P WAVE • SINE-WAVE PATTERN (QRS COMPLEX MERGES WITH THE T WAVE)
Hyperkalemia- Diagnosis • ANAMNESIS • PHYSICAL EXAMINATION • CHECK FOR: pH, urea and creatinine, glucose, markers of tissue damage (LDH, CPK), ECG.