Download
1 / 32
• 360 likes • 640 Views
Section III.Disturbance of Potassium Balance. Potassium Balance (1) Content and distribution (2) Function of potassium (3) Regulation of K + balance Hypokalemia Hyperkalemia. 1. Potassium Balance (1) Content and distribution.

E N D
Section III.Disturbance of Potassium Balance Potassium Balance (1) Content and distribution (2) Function of potassium (3) Regulation of K+ balance Hypokalemia Hyperkalemia
1. Potassium Balance(1) Content and distribution • The adult body contains about 45 mmol/Kg of BW. • About 98% of potassium is within the cells, • [K +] i= 140~160 mmol/L. • About 2% of K + is in the ECF, • [K +]e = 3.5~5.5 mmol/L. • 3/4 of the intracellular K+ is in muscle cells.
There are two forms of existence: • (1) free state of potassium, K+, • (2) the K combining to protein and glycogen. • Both are exchangeable. • (Na+)
(2) Function of potassium • 1) Metabolism • 2) Membrane potential • 3) Regulation of pH • 4) Osmotic pressure of ICF
1) Metabolism • (a) K+ is required for the activity of some intracellular enzymes e.g. the enzyme for ATP production. • (b) K+ is involved in anabolism. • 1 g of glycogen contents 0.33~0.45 mmol, • The K+ moves into cells with glucose, during the synthesis of glycogen. • 1 g of protein needs 30 mmol of K+.
2) Membrane potential • The ratio of the intracellular to the extracellular potassium concentration • ([K+]i∕[K+]e) constitutes the cellular resting membrane potential. • Minimal change of [K+]e may affect the membrane potential obviously. • K+ is important for normal neuromuscular irritability.
3) Regulation of pH • Exchange of K+ and H+ crossing the cell membrane is important for acid-base balance. • Changes of K+ concentration will lead to the changes of pH. • When K+ moves out of the cells, H+ will move into the cells as an exchange for electrical neutrality. More H+ will lead to acidosis.
4) Osmotic pressure • Potassium ion is the major intracellular cation, so K+ is important in the formation of osmotic pressure in the cell. • To keep the volume of ICF.
(3) Regulation of K+ balance • 1) Equilibrium of K+ in ICF and ECF • 2) Balance of intake and excretion • K excretion in kidney • K excretion in colon
1) Equilibrium of K+ in ICF and ECF (transcellular potassium movement) • Equilibrium means to keep • [K+]i= 140~160 mmol/L; • [K+]e = 3.5~5.5 mmol/L
Significance : After intake a bottle of orange juice (40 mmol/L of K+), if all K+ stays in ECF, the [K+]e=4.5+2.4=6.9 mmol/L, which will lead to abnormal ECG. Abnormal ECG means the heart muscle is injured. If all K+ is transported into ICF, the [K+]i=160+1.2=161.2 mmol/L. Then the excessive K+ will be eliminated within several hours in the urine.
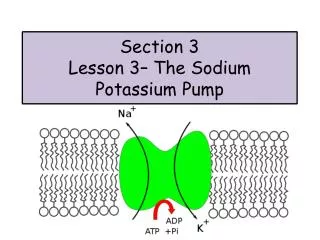
Mechanism to keep the equilibrium: The basic mechanism to the balance is “leak and pump”. (Integrity of cell membrane and function of Na+-K+ pump)
钾的跨细胞转移调节 细胞内液[K+] 140-160mmo1/L Na+ - K+泵(泵) K+ K+ 细胞外液[K+] 4.2mmol/L Na+ Na+ K+ K+ K+通道(漏) K+细胞内外移动的泵一漏机制 (Pump-leak mechanism)
钾代谢紊乱 【影响钾的跨细胞转移的主要因素】 可直接刺激Na+-K+泵活性,影响钾转移主要激素。 胰岛素 肾上腺素通过cAMP机制激活Na+-K+泵活性,肾上腺能神经激活是促K+自细胞内移出。 儿茶酚胺 ECF [H+]↑, H+入细胞内,细胞内K+外移。ECF每0.1 pH变化大约引起0.6mmol/L血清钾变化 ECF [K+] ICF [K+] 140-160mmo1/L 酸碱平衡状态 渗透压 ECF 渗透压↑ ↑ ,使细胞内K+外移。 运动 ECF [K+] 4.2mmol/L
(a) Changes of pH A decrease in pH of 0.1 units usually elevates the serum [K+] by about 0.6 mmol/L. (alkalosis: pH ↑ 0.1, [K+] ↓ 0.6 mmol/L)
(b) Extracellular K+ concentration • A high [K+]e will stimulate the activity of Na+-K+ pump. • A low [K+]e will do in the converse way.
(c) Total K quantity in the body • When the total quantity of K in the body reduces, the loss of intracellular K+ is more than extracellular K+, but the ratio of extracellular K+ loss is more than intracellular K+ loss. • When the total quantity of K in the body increases , the increase of intracellular K+ is more than extracellular K+, but the ratio of extracellular K+ increase is more than intracellular K+ increase.
(d) Regulation of hormone Insulin promotes the movement of K+ into the liver cells and skeletal muscle cells by increasing sodium-potassium ATPase activity. The β-adrenergic agonists also elevate Na+ -K+ pump activity to enhance K+ entry. The α-adrenergic agents enhance the K+ transport out of cells. Epinephrine stimulates α-recepter first,then β-recepter. (K+ )
(e) Metabolism(anabolism; catabolism) Increased anabolism (AA protein, glucose glucogen) elevates the [K+]i. Increased catabolism (protein AA, glucogen glucose) reduces the [K+]i.
f) Increased smotic pressure of ECF leads to increased [K+]e. • Increased osmolality of extracellular fluid draws the water out of cells with K+. Decreased water in the cells elevates the [K+]i. The difference [K+]iand [K+]e increases, which leads to the shift of K+ out of cells increases.
(g) Exercise • Exercise can promote K shift out of cells through: (1) opening of ATP-dependent K+ channels 与电压依赖型的钾离子通道不同,也与依赖钙离子的钾离子通道不同,,KATP通道主要受细胞内的ATP浓度调节。在生理条件下细胞内ATP浓度约为3-4 mmol.L-1, KATP通道基本处于关闭状态。只有当心肌细胞发生缺血缺氧,能量耗竭,胞内ATP浓度低于0.2 mmol.L-1时通道开放,K+外流, 游离ATP是KATP通道最强而有效的内源性阻断剂,其主要功能有:(1)舒张血管,包括外周血管和冠状动脉。主要由于KATP激活,K+外流,细胞复极化加速,使动作电位时程缩短,Ca2+内流减少,血管舒张。 (2)Ca2+内流减少,使心肌收缩力减弱,降低心肌氧耗,产生心脏保护作用。 (2) decrease Na+ -K+ ATPase activity due to ATP depletion.
(h) Integrity of cellular membrane • “Leak” indicates the moving of K+ out of the cell according to the gradient of [K+ ] between ICF and ECF, without expending ATP. • Leaking leads to the tendency to reduce the [K+]i. When the cell membrane is injured, the permeability of cell membrane to K+ is increased. More K+ move from cells into ECF.
2) Balance of intake and excretion • (a) Intake: The common foods, like lean meat, milk and fruits content a lot of potassium. • The average diet contains 60~100 mmol of potassium per day, which is enough for the daily body requirement. 90% of potassium in food is absorbed in small intestine.
(b) Excretion • ① Via kidney • About 90% or more potassium is eliminated from kidney. (12字) • The more K we eat, the more K is eliminated from kidneys. When the intake of potassium is decreased, the elimination from urine is decreased. • If no potassium intake, the kidneys will still secrete small amount of potassium (20~15 mmol/day). (Na+?)
Potassium is freely filtered at the glomerulus. Almost all the potassium filtered is reabsorbed in proximal tubules via active transport. In loop of Henle: via Na+-K+-2Cl-contransporter. • Most of the potassium in the urine is secreted from distal tubules and collecting ducts. • No decrease of K+ filtration except severe reduction of GFR.
a) aldosterone • Aldosterone activates pump (Na+ /K+ pump) in basolateral membrane, the K+ transport from peritubular interstitial fluid into renal tubular cells will increase. • Aldosterone increases the permeability of lumenal membrane, the K+ transport from renal tubular cells into tubules (urine) will increase. • (C)Regulation of renal loss in renal distal tubules and collecting ducts,
b) High [K+]e High [K+]e activates pump (Na+ /K+ pump) in basolateral membrane, the K+ transport from peritubular interstitial fluid into renal tubular cells will increase. High [K+]e increases the permeability of lumenal membrane, the K+ transport from renal tubular cells into tubules (urine) will increase. High [K+]edecreases the [K+] difference between renal tubular cells and peritubular interstitial fluid, then decrease the back-flow of K+ from tubule.
c) Volume and flow rate of urine in distal tubules and collecting ducts Increased volume and flow rate of urine in distal tubules and collecting ductsreduce the [K+], increase the difference between the [K+] in urine and in tubule cells, increase the excretion of K.
d) Acid-base balance • In acute acidosis, increased [H+] suppresses Na+-K+-ATPase, and the excretion of K+ decreases. • In alkalosis the excretion of K+ increases. • In chronic acidosis, the dominant effect is that increased [H+] suppresses the reabsorption of water and sodium in proximal tubule cells, urine volume increases, excretion of K+ increases.
e) Electric field If more negative charges in tubular fluid, more K+ will be excreted.
② Via intestinal tract K excretion in colon • 10% of K is excreted through the colon. The epithelial cells are just as the principal cells in the collecting duct, and affected by aldosterone. • K+ excretion via colon will increase in renal failure. • GFR↓↓↓ K excretion in colon to 1/3 of intake .
③ Via sweating • Generally speaking, the loss of K+ with sweat is neglectful (5~10 mmol/L). This kind of loss may be significant some time (in plenty of sweat).