Download
1 / 1
10 likes | 104 Views
Incidence of lipodystrophy and metablic syndrome after the initiation of combined antiretroviral therapy (cART) in Sub-Saharan cART-naïve patients

E N D
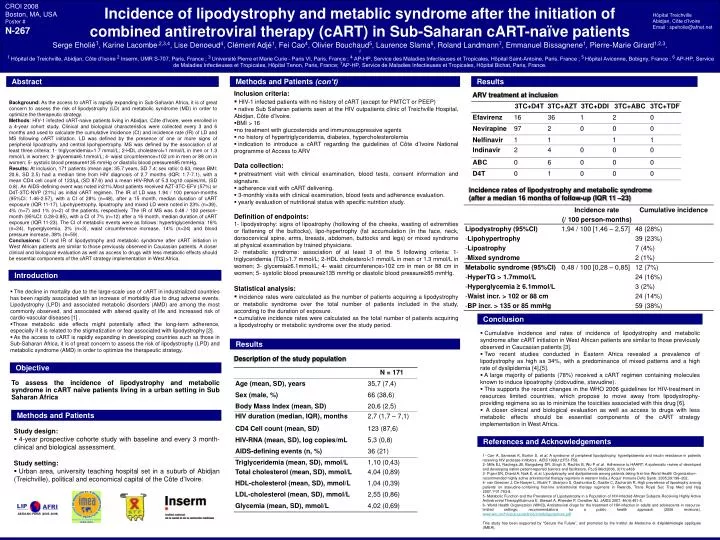
Incidence of lipodystrophy and metablic syndrome after the initiation of combined antiretroviral therapy (cART) in Sub-Saharan cART-naïve patients Serge Eholié1, Karine Lacombe,2,3,4, Lise Denoeud4, Clément Adjé1, Fei Cao4, Olivier Bouchaud5, Laurence Slama6, Roland Landmann7, Emmanuel Bissagnene1, Pierre-Marie Girard1,2,3. 2 1 Hôpital de Treichville, Abidjan, Côte d’Ivoire 2 Inserm, UMR S-707, Paris, France ; 3 Université Pierre et Marie Curie – Paris VI, Paris, France ; 4 AP-HP, Service des Maladies Infectieuses et Tropicales, Hôpital Saint-Antoine, Paris, France ; 5 Hôpital Avicenne, Bobigny, France ; 6 AP-HP, Service de Maladies Infectieuses et Tropicales, Hôpital Tenon, Paris, France;7AP-HP, Service de Maladies Infectieuses et Tropicales, Hôpital Bichat, Paris, France. CROI 2008 Boston, MA, USA Poster # N-267 Hôpital Treichville Abidjan, Côte d’Ivoire Email : speholie@afnet.net Abstract Methods and Patients (con’t) Results • Inclusion criteria: • HIV-1 infected patients with no history of cART (except for PMTCT or PEEP) • native Sub Saharan patients seen at the HIV outpatients clinic of Treichville Hospital, Abidjan, Côte d’Ivoire. • BMI > 16 • no treatment with glucosteroids and immunosuppressive agents • no history of hypertriglyceridemia, diabetes, hypercholesterolemia • indication to introduce a cART regarding the guidelines of Côte d’Ivoire National programme of Access to ARV Data collection: • pretreatment visit with clinical examination, blood tests, consent information and signature. • adherence visit with cART delivering. • 3-monthly visits with clinical examination, blood tests and adherence evaluation. • yearly evaluation of nutritional status with specific nutrition study. Definition of endpoints: • 1- lipodystrophy: signs of lipoatrophy (hollowing of the cheeks, wasting of extremities or flattening of the buttocks), lipo-hypertrophy (fat accumulation (in the face, neck, dorsocervical spine, arms, breasts, abdomen, buttocks and legs) or mixed syndrome at physical examination by trained physicians. • 2- metabolic syndrome: association of at least 3 of the 5 following criteria: 1- triglyceridemia (TG)>1.7 mmol/L; 2-HDL cholesterol<1 mmol/L in men or 1.3 mmol/L in women; 3- glycemia≥6.1mmol/L; 4- waist circumference>102 cm in men or 88 cm in women; 5- systolic blood pressure≥135 mmHg or diastolic blood pressure≥85 mmHg. Statistical analysis: • incidence rates were calculated as the number of patients acquiring a lipodystrophy or metabolic syndrome over the total number of patients included in the study, according to the duration of exposure. • cumulative incidence rates were calculated as the total number of patients acquiring a lipodystrophy or metabolic syndrome over the study period. ARV treatment at inclusion Background: As the access to cART is rapidly expanding in Sub-Saharan Africa, it is of great concern to assess the risk of lipodystrophy (LD) and metabolic syndrome (MD) in order to optimize the therapeutic strategy. Methods: HIV-1 infected cART-naive patients living in Abidjan, Côte d’Ivoire, were enrolled in a 4-year cohort study. Clinical and biological characteristics were collected every 3 and 6 months and used to calculate the cumulative incidence (CI) and incidence rate (IR) of LD and MS following cART initiation. LD was defined by the presence of one or more signs of peripheral lipoatrophy and central lipohypertrophy. MS was defined by the association of at least three criteria: 1- triglyceridemia>1.7 mmol/L; 2-HDL cholesterol<1 mmol/L in men or 1.3 mmol/L in women; 3- glycemia≥6.1mmol/L; 4- waist circumference>102 cm in men or 88 cm in women; 5- systolic blood pressure≥135 mmHg or diastolic blood pressure≥85 mmHg. Results: At inclusion, 171 patients (mean age: 35.7 years, SD 7.4; sex ratio: 0.63, mean BMI: 20.6, SD 2.5) had a median time from HIV diagnosis of 2.7 months (IQR: 1.7-7.1), with a mean CD4 cell count of 123/μL (SD 87.6) and a mean HIV-RNA of 5.3 log10 copies/mL (SD 0.8). An AIDS-defining event was noted in21%.Most patients received AZT-3TC-EFV (57%) or D4T-3TC-NVP (21%) as initial cART regimen. The IR of LD was 1.94 / 100 person-months (95%CI: 1.46-2.57), with a CI of 28% (n=48), after a 15 month, median duration of cART exposure (IQR 11-17). Lipohypertrophy, lipoatrophy and mixed LD were noted in 23% (n=39), 4% (n=7) and 1% (n=2) of the patients, respectively. The IR of MS was 0.48 / 100 person-month (95%CI: 0.28-0.85), with a CI of 7% (n=12) after a 16 month, median duration of cART exposure (IQR 11-23). The CI of metabolic events were as follows: hypertriglyceridemia: 16% (n=24), hyperglycemia, 2% (n=3), waist circumference increase, 14% (n=24) and blood pressure increase, 38% (n=59). Conclusions: CI and IR of lipodystrophy and metabolic syndrome after cART initiation in West African patients are similar to those previously observed in Caucasian patients. A closer clinical and biological evaluation as well as access to drugs with less metabolic effects should be essential components of the cART strategy implementation in West Africa. Incidence rates of lipodystrophy and metabolic syndrome (after a median 16 months of follow-up (IQR 11 –23) Introduction • The decline in mortality due to the large-scale use of cART in industrialized countries has been rapidly associated with an increase of morbidity due to drug adverse events. Lipodystrophy (LPD) and associated metabolic disorders (AMD) are among the most commonly observed, and associated with altered quality of life and increased risk of cardio-vascular diseases [1] . • Those metabolic side effects might potentially affect the long-term adherence, especially if it is related to the stigmatization or fear associated with lipodystrophy [2]. • As the access to cART is rapidly expanding in developing countries such as those in Sub-Saharan Africa, it is of great concern to assess the risk of lipodystrophy (LPD) and metabolic syndrome (AMD) in order to optimize the therapeutic strategy. Conclusion • Cumulative incidence and rates of incidence of lipodystrophy and metabolic syndrome after cART initiation in West African patients are similar to those previously observed in Caucasian patients [3]. • Two recent studies conducted in Eastern Africa revealed a prevalence of lipodystrophy as high as 34%, with a predominance of mixed patterns and a high rate of dyslipidemia [4],[5]. • A large majority of patients (78%) received a cART regimen containing molecules known to induce lipoatrophy (zidovudine, stavudine). • This supports the recent changes in the WHO 2006 guidelines for HIV-treatment in resources limited countries, which propose to move away from lipodystrophy-providing regimens so as to minimize the toxicities associated with this drug [6]. • A closer clinical and biological evaluation as well as access to drugs with less metabolic effects should be essential components of the cART strategy implementation in West Africa. Results Description of the study population Objective To assess the incidence of lipodystrophy and metabolic syndrome in cART naïve patients living in a urban setting in Sub Saharan Africa Methods and Patients • Study design: • 4-year prospective cohorte study with baseline and every 3 month- clinical and biological assessment. Study setting: • Urban area, university teaching hospital set in a suburb of Abidjan (Treichville), political and economical capital of the Côte d’Ivoire. References and Acknowledgements 1- Carr A, Samaras K, Burton S, et al.A syndrome of peripheral lipodystrophy, hyperlipidaemia and insulin resistance in patients receiving HIV protease inhibitors. AIDS 1998,12:F51-F58. 2- Mills EJ, Nachega JB, Bangsberg DR, Singh S, Rachlis B, Wu P et al. Adherence to HAART: A systematic review of developed and developing nation patient-reported barriers and facilitators. PLoS Med 2006, 3(11):e438 3- Pujari SN, Dravid A, Naik E, et al. Lipodystrophy and dyslipidaemia among patients taking first-line World Health Organization–recommended highly active antiretroviral therapy regimens in western India.J Acquir Immune Defic Syndr. 2005;39:199–202. 4- van Griesven J, De Naeyer L, Mushi T, Ubarijoro S, Gashumba D, Gazille C, Zachariah R. High prevalence of lipoatrophy among patients on stavudine-containing first-line antiretroviral therapy regimens in Rwanda. Trans Royal Soc Trop Med and Hyg 2007,1°01:793-8. 5- Metabolic Function and the Prevalence of Lipodystrophy in a Population of HIV-Infected African Subjects Receiving Highly Active Antiretroviral TherapyMutimura E, Stewart A, Rheeder P, Crowther NJ. JAIDS 2007, 46(4):451-5. 6- World Health Organization (WHO). Antiretroviral drugs for the treatment of HIV-infection in adults and adolescents in resource-limited settings; recommendations for a public health approach (2006 revisions). www.who.int/hiv/pub/guidelines/artadultguidelines.pdf This study has been supported by “Secure the Future”, and promoted by the Institut de Medecine et d’épidémiologie appliquée (IMEA). LIP AFRI ABIDJAN–PARIS (2005–2009)