Download
1 / 12
120 likes | 329 Views
LONG-TERM OUTCOME OF DRUG-ELUTING STENTS COMPARED WITH BARE METAL STENTS IN ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION Results of the Paclitaxel- or Sirolimus-Eluting Stent Versus Bare Metal Stent in Primary Angioplasty (PASEO) Randomized Trial.

E N D
LONG-TERM OUTCOME OF DRUG-ELUTING STENTS COMPARED WITH BARE METAL STENTS IN ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION Results of the Paclitaxel- or Sirolimus-Eluting Stent Versus Bare Metal Stent in Primary Angioplasty (PASEO) Randomized Trial Emilio Di Lorenzo1, Rosario Sauro1, Attilio Varricchio1, Giannignazio Carbone1, Giuliana Cortese2, Michele Capasso1, Tonino Lanzillo1, Fiore Manganelli1, Ciro Mariello1, Francesco Siano1, Maria Rosaria Pagliuca1, Giovanni Stanco1, Giuseppe Rosato1, Giuseppe De Luca3 1Department of Cardiology and Cardiovascular Surgery, A.O.R.N. S.G. Moscati, Avellino, Italy 2Department of Statistical Sciences, University of Padova, Italy 3Division of Cardiology, Ospedale “Maggiore della Carità,” Eastern Piedmont University, Italy.
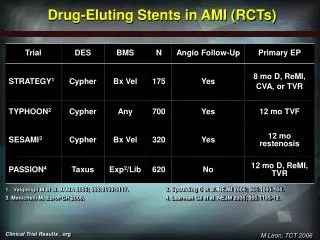
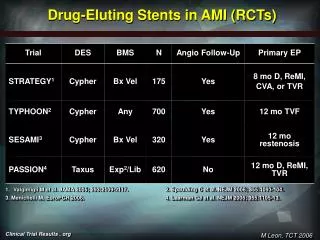
BACKGROUND • Routine stent implantation has been advocated for patients with acute myocardial infarction (MI) referred for primary angioplasty, with superior results compared to balloon dilation. (Stone GW et al N Engl J Med. 2002;346:957–966) (Keeley EC et al Lancet 2003; 361: 13-20) (Antoniucci D et al Circulation. 2004;109: 1704–1706) • However, the late clinical efficacy is still hampered by the occurrence of in-stent restenosis and the need for repeat intervention. (Suryapranata H, Heart. 2005; 91:641– 645) (De Luca G et al Int J Cardiol. 2008;126:37– 44) • Several randomized trials have shown that drug-eluting stents (DES) are associated with a significant reduction in restenosis and TVR in both elective and STEMI patients compared with BMS (Kastrati A et al Eur Heart J. 2007;28:2706 –2713) (De Luca G et al Int J Cardiol. 2009;133:213–222) • No data have been reported on long-term results of DES compared with BMS in STEMI patients
AIM OF THE STUDY • The Paclitaxel or Sirolimus-Eluting Stent Versus Bare Metal Stent in Primary Angioplasty (PASEO) randomized trial evaluates the benefits of sirolimus-eluting stents (SES) and paclitaxel-eluting stents (PES) compared with bare metal stents (BMS) in patients undergoing primary angioplasty for STEMI at short- and long-term follow-up.
STUDY DESIGN • Inclusion criteria: chest pain lasting >30 minutes, ST-segment elevation of >1 mm in >2 contiguous ECG leads or with presumably new left bundle-branch block, and hospital admission within 12 hours from symptom onset. • Open-label randomization was performed in the catheterization laboratory after initial angiography by the treating physician when eligibility criteria were met. • Exclusion criteria: active internal bleeding or a history of bleeding diathesis within the previous 30 days; a history of intracranial hemorrhage, intracranial neoplasm, arteriovenous malformation, or aneurysm; known allergy to sirolimus, paclitaxel, heparin, aspirin, or clopidogrel; a history of stroke within 30 days or any history of hemorrhagic stroke; major surgical procedure or severe physical trauma within the previous month; history, symptoms, or findings suggestive of aortic dissection; thrombolytic/fibrinolytic therapy within 24 hours; history of thrombocytopenia; and hemorrhagic retinopathy; Patients on warfarin or acenocoumarol with an international normalized ratio >2, pregnant patients and a vessel site <2.25 mm.
STUDY DESIGN 323 STEMI PATIENTS ASSESSED FOR ELIGIBILITY 53 patients excluded because of exclusion criteria or refusal to partecipate 270 PATIENTS FINALLY RANDOMIZED 90 ASSIGNED TO Sirolimus Eluting Stent (SES) 90 ASSIGNED TO Paclitaxel Eluting Stent (PES) 90 ASSIGNED TO Bare Metal Stent (BMS)
END POINTS • Primary end point: • Target lesion revascularization (TLR) at the 1-year follow-up. • Secondary end points • Death and/or reinfarction • In-stent thrombosis defined according to the Academic Research Consortium definition • Major adverse cardiac events (MACEs) (combined death and/or reinfarction and/or TLR) at the long-term (up to 4 to 6 years) follow-up. • All deaths were considered cardiac unless an unequivocal noncardiac cause could be identified. • Recurrent MI was defined as recurrence on anginal symptoms with typical ECG changes and an increase above the upper limit of normal of creatine kinase-MB or troponin. • The indication for a second intervention had to be substantiated by symptoms or by ECG or scintigraphic evidence of ischemia at rest or during exercise. • Subsequent revascularization of other coronary arteries did not constitute an end point. • All events were reviewed by 2 cardiologists blinded to treatment assignment.
Baseline demographic and clinical characteristics of the three groups of patients
Angiographic and procedural characteristics of the three groups of patients
*p<0.05 vs BMS # p<0.05 vs BMS 30 20 1 year outcome # * % 10 * # 0 TLR Death reMI MACEs IST 40 30 3 year outcome BMS * # % 20 PES * # 10 SES 0 TLR Death reMI MACEs IST 50 40 3 to 6 year outcome * # 30 % 20 # * 10 0 TLR Death reMI MACEs IST
3 to 6 years Clinical Outcomes (median 4.3 years) SES vs BMS PES vs BMS BMS N=90 PES N=90 SES N=90 HR P HR P Death, (%) 13.3 8.9 7.8 0.66 0.36 0.56 0.23 reMI, (%) 14.4 8.9 10 0.59 0.25 0.66 0.34 reMI and/or death, (%) 23.3 17.8 16.7 0.74 0.36 0.68 0.26 TLR, (%) 22.2 6.7 5.6 0.27 0.005 0.22 0.003 TLR and/or death, (%) 31.1 15.6 13.3 0.46 0.017 0.38 0.005 TVR, (%) 23.3 7.8 6.7 0.30 0.006 0.25 0.003 TVR and/or death, (%) 32.2 16.7 14.4 0.47 0.018 0.40 0.005 IST, (%) 8.9 5.6 4.4 0.64 0.44 0.48 0.23 Definite, (%) 1.1 1.1 1.1 Probable, (%) 2.2 1.1 1.1 Possible, (%) 5.6 3.3 2.2 IST and/or death, (%) 14.4 10 10 0.71 0.42 0.66 0.34 MACEs, (%) 40.0 23.3 22.2 0.52 0.016 0.48 0.009
CONCLUSIONS • The main finding of the present study is that PES and SES are more effective than BMS mainly because of a reduction in TLR, with no excess risk of thrombotic complications. • Our study demonstrates the long-term safety and benefits of both SES and PES compared with BMS. • Of relevance, unlike the vast majority of randomized trials conducted to date, the superiority of SES and PES was observed without the use of routine angiographic follow-up in our trial.
MAJOR LIMITATIONS OF STUDY • Because of a relatively late randomization strategy (after initial angiography), patients have for the most part been selected; • Despite long-term follow-up data, as a result of the relatively small sample size, this trial cannot provide definite conclusions on DES safety in terms of death and reinfarction, which we hope will be provided by large randomized trials.