Download
1 / 37
370 likes | 684 Views
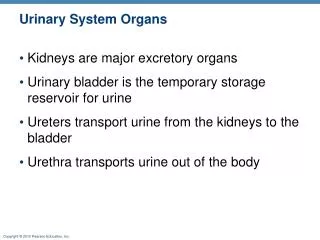
老人尿失禁的照護技巧 The Techniques of Caring the Aging with Urinary Incontinence. 王炯珵 恩主公醫院泌尿科 Chung Cheng Wang Department of Urology En Chu Kong Hospital. State of the Science on Urinary Incontinence.

E N D
老人尿失禁的照護技巧The Techniques of Caring the Aging with Urinary Incontinence 王炯珵 恩主公醫院泌尿科 Chung Cheng Wang Department of Urology En Chu Kong Hospital
State of the Science on Urinary Incontinence • Nurses have in their toolboxes some help for first-line UI intervention and screening [Diane Newman, 2002 July] • The first priority is to increase awareness among nurses. [Mary Palmer, 2003AJN] • Noninvasive behavioral interventions can be effective in long-term care setting • But staff compliance was problematic [Palmer MH 1997]
Epidemiology • 20 million American have UI [Abram P 2002] • 22% of women aged 65 and older had UI in daily life [Tseng 2000] • More than 50% of nursing home residents [Fantl J,1996]
Differences in Gender • Female: male = 2:1[Hunskaar S 2001] • stress or mixed UI: female • Pure urge UI: equal • Postvoid dribbling, nocturnal enuresis: male [Temml C 2000] • Women were more likely to regularly use strategies for UI management [Johnson TM 2000]
Risk Factors in Women • Gravidity and parity • One vaginal birth: 2.5 times for UI [Nygaard IE 1994] • Breech presentation, use of forceps, tearing, central episiotomy, oxytocin • Pelvic organ prolapse • Gynecologic surgery • Menopause • Obesity [Roe B 1999]
Risk Factors in Men • A history of radical or transurethral prostatectomy[Umlauf 1996] • The first year of admission to a long-term care facility [Palmer MH 1991] • Causes of urge UI in elderly men: UTI, prostate inflammation, bowel dysfunction [Herzog AR 1990]
UI in the Frail Elderly • Frail: decline in physical activity [Bortx WM 2002] • Frail elderly: >65, UI, can not go out without assistance, dementia, admitted to a long-term care facility [Fonda D 1998]
Risk Factors in Frail Elderly • Multiple medical morbidities • Immobility • Cognitive impairment (dementia)
Screening • Routine assessment for UI can be easily incorporated into the general history questions [Feneley RC BJU 1997] • Screening by risk factors • Urge UI + Nocturia >2 + daytime voiding frequency of < 2hr = 90% detrusor overactivity on UDS [Gray M, 2001]
Assessment of UI in the Frail Older Adult • History and symptom assessment • Clinical and physical assessment • Environmental assessment • Identify possible diagnosis or clinical impression
Potential Reverse Causes • Delirium, dementia, depression • Infection (UTI) • Atrophic vaginitis • Pharmaceuticals • Psychological, Pain • Excess fluid (polyuria, edema) • Restricted mobility • Stool (constipation)
Behavioral Therapy • AHCPR guideline • Bladder training: strongly recommended for urge and mixed incontinence and also recommended for stress UI • Pelvic floor rehabilitation: strongly recommended for stress UI • The first line of treatment[Fantl J 1996]
Nonpharmacologic Management of UI in Adults • Lifestyle or risk factors modification • Scheduled voiding regimens • Pelvic floor muscle rehabilitation • Anti-incontinence devices • Supportive interventions
Lifestyle Modification • Reduce risk factors • Stress UI: smoking cessation,change body position [Norton PA 1994], weight reduction [Deitel M 1988] • Constipation: good bowel hygiene • Urge UI: caffeine reduction, selected dietary and fluid modification • No study support: bladder irritants, alcohol [Wyman JF 2000]
Nonpharmacologic Management of UI in Adults • Lifestyle or risk factors modification • Scheduled voiding regimens • Pelvic floor muscle rehabilitation • Devices • Supportive intervention
Scheduled Voiding Regimens • Timed voiding • Habit retraining • Patterned urge response toileting • Prompted voiding • Bladder training
Nonpharmacologic Management of UI in Adults • Lifestyle or risk factors modification • Scheduled voiding regimens • Pelvic floor muscle rehabilitation • Anti-incontinence devices • Supportive intervention
Pelvic Floor Muscle Rehabilitation • Pelvic floor muscle exercise • Vaginal weight training • Biofeedback • Electric stimulation • Magnetic stimulation
Nonpharmacologic Management of UI in Adults • Lifestyle or risk factors modification • Scheduled voiding regimens • Pelvic floor muscle rehabilitation • Anti-incontinence devices • Supportive intervention
Anti-incontinence Device • Intravaginal support device • External occlusive device • Intraurethral occlusive device • Complex valved catheter • External collection device • Urethral catheter
Intravaginal Support Device • Pessary • Support the bladder neck, relieve minor pelvic prolapse and change pressure transmission • Stress UI • Estrogen replacement for postmenopausal women
External Occlusive Device • A small single-use device that covers the urethral meatus for women • A penile clamp for men • Need good manual dexterity • Complication: periurethral irritation or penile erosion
Intraurethral Occlusive Device • Urethral plug • A small single-use device that is worn in the urethra to provide mechanical obstruction • Used for stress UI in cognitively intact patient • Complication: urethral irritation, hematuria, UTI or migrate into bladder
Complex Valved Catheter • Intraurethral occlusive device with a unidirectional valve • Left indwelling for long period • Must be inserted and removed by a clinician • Being test for female stress UI, overflow UI • Complication: urethral irritation, hematuria, UTI
External Collection Device • Condom catheter with leg bag • Used in men with urge, stress and overflow UI and in those with functionally impairment • More comfortable, less painful and less restrictive than use of an indwelling catheter [Saint S 1999] • Risk for UTI, penile skin marceration
Urethral Catheters • Disposable, single-use catheter and indwelling catheters • Used for overflow UI • Bedbound, mobility impairment and severe UI • Clean intermittent catheterization is the standard care of spinal cord injury [Perrouin-Verbe B 1995]
Indications for Long-term Indwelling Catheters • Persistent overflow UI, symptomatic UTI or kidney disease • Surgical or pharmacologic intervention failed • Contraindication for CIC • Changes of bedding, clothing and absorbent products may be painful or disruptive for p’t with an irreversible medical condition • Not healed grade 3-4 pressure ulcers • Patients live alone without a caregiver
Nonpharmacologic Management of UI in Adults • Lifestyle or risk factors modification • Scheduled voiding regimens • Pelvic floor muscle rehabilitation • Anti-incontinence devices • Supportive intervention
Supportive Interventions • Toileting substitutes and other environmental modifications • Physical and occupational therapy • Absorbent products
Toileting Substitutes and Other Environmental Modifications • Urinals, bedside commodes, elevated toilet seats • Used for patients with mobility impairment that make it difficult to reach a toilet in a timely fashion
Physical and Occupational Therapy • Gait and strength training • Used for frail older patients with mobility or manual dexterity impairments that make it difficult to reach a toilet and disrobe in a timely fashion
Absorbent Products • Reusable and disposable pads and pants system • Some products contain a polymer that absorbs urine and binds with urine, changing it into gel[Newman D 2002] • Used for all types of incontinence • But never be used solely for the convenience of the caregiver
Behavioral Therapy in Frail Elders • Adequate fluid intake • Bowel regularity • Perineal hygiene • Voiding every 2 to 4 hours • Avoid caffeine in urge UI • Toileting programs
Skin Care • Perineal hygiene after toileting • Skin dryness • Comfortable clothes • Skin ulcer: isolation cream, Duoderm, Comfeel
Prevention of Excess Disability • The two primary risk factors for UI among the frail elderly are immobility and cognitive impairment • Tailored programs that enhance physical mobility and cognitive function [Schnelle J 2000] • Optimal management of acute and chronic illness • Environmental modification • Prosthetic support [Weindrug R 1991]
Algorithm -- I • Three-day bladder record, measure RU • Determine which type of UI • What trigger it • Individual care plans • Four goals: fewer incontinence episodes, daytime continence, 24-hour continence, the prevention of skin breakdown and odor
Algorithm -- II • Behavioral interventions • Ambulatory assistance • Cognitively intact PFM training • Passive exercise • Goal one to goal three • Goal four is reserved for comatose or very debilitated patients