Download
1 / 1
10 likes | 227 Views
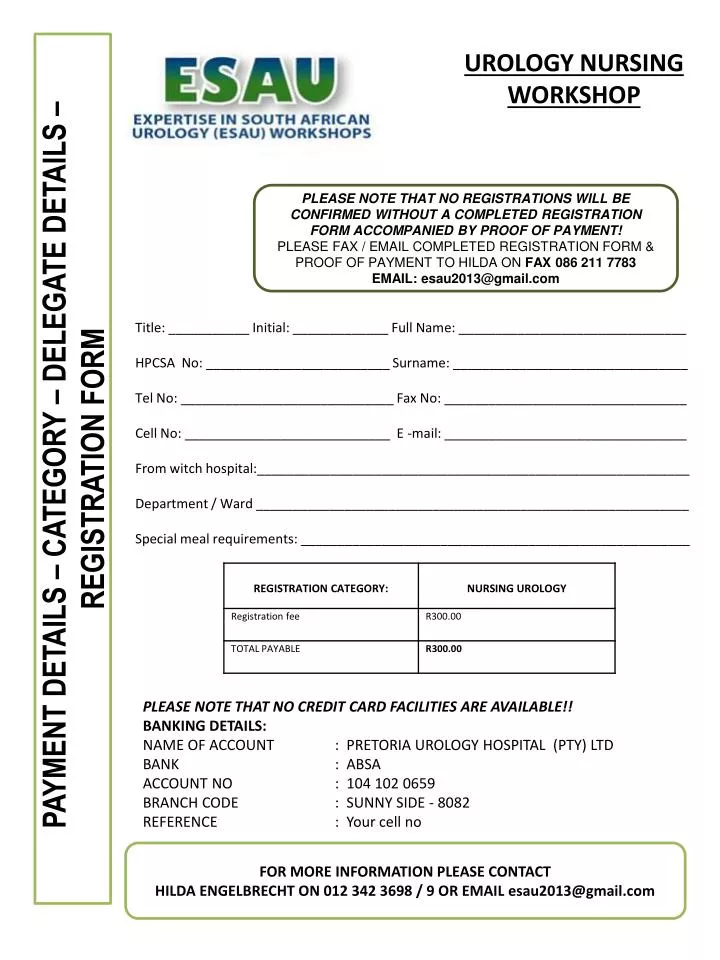
UROLOGY NURSING WORKSHOP. PLEASE NOTE THAT NO REGISTRATIONS WILL BE CONFIRMED WITHOUT A COMPLETED REGISTRATION FORM ACCOMPANIED BY PROOF OF PAYMENT! PLEASE FAX / EMAIL COMPLETED REGISTRATION FORM & PROOF OF PAYMENT TO HILDA ON FAX 086 211 7783 EMAIL: esau2013@gmail.com.

E N D
UROLOGY NURSING WORKSHOP • PLEASE NOTE THAT NO REGISTRATIONS WILL BE CONFIRMED WITHOUT A COMPLETED REGISTRATION FORM ACCOMPANIED BY PROOF OF PAYMENT! • PLEASE FAX / EMAIL COMPLETED REGISTRATION FORM & PROOF OF PAYMENT TO HILDA ON FAX 086 211 7783 • EMAIL: esau2013@gmail.com Title: ___________ Initial: _____________ Full Name: _______________________________ HPCSA No: _________________________ Surname: ________________________________ Tel No: _____________________________ Fax No: _________________________________ Cell No: ____________________________ E -mail: _________________________________ From witch hospital:___________________________________________________________ Department / Ward ___________________________________________________________ Special meal requirements: _____________________________________________________ PAYMENT DETAILS – CATEGORY – DELEGATE DETAILS – REGISTRATION FORM PLEASE NOTE THAT NO CREDIT CARD FACILITIES ARE AVAILABLE!! BANKING DETAILS: NAME OF ACCOUNT : PRETORIA UROLOGY HOSPITAL (PTY) LTD BANK : ABSA ACCOUNT NO : 104 102 0659 BRANCH CODE : SUNNY SIDE - 8082 REFERENCE : Your cell no FOR MORE INFORMATION PLEASE CONTACT HILDA ENGELBRECHT ON 012 342 3698 / 9 OR EMAIL esau2013@gmail.com