Download
1 / 99

E N D
Patients with APS are often treated with an injectable anticoagulant called heparin. In some cases, the heparin is given into a vein while the patient is in the hospital. In other cases, heparin is injected under the skin. Or taking a daily small dose of aspirin can help a woman be more fertile
The Various Forms of Triglycerides and PhospholipidsFound in the Cell
phospholipid bilayersOne structure that can result when phospholipids are suspended in water is shown below. A bilayer of phospholipids forms a sphere in which water is trapped inside. The hydrophilic phosphate regions interact with the water inside and outside of the sphere. The fatty acids of the phospholipids interact and form a hydrophobic center of the bilayer.
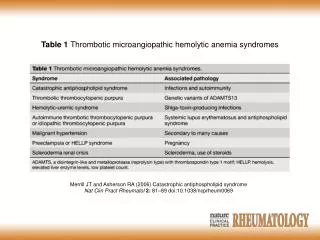
Updated Sapporo classification criteria for antiphospholipid syndrome (APS
Anti –phospholipid syndrome • Antiphospholipid syndrome (APS) is an autoimmune disease associated with frequent clotting in arteries and veins and/or miscarriages. The clotting results from the presence of proteins in the blood called anti-phospholipid autoantibodies formed against the person’s own tissues. In circulation, these autoantibodies are able to interfere with some mechanisms of coagulation leading to clot formation or thrombosis.
Anti –phospholipid syndrome • Virtually any system can be affected including: • * Peripheral artery thrombosis, deep venous thrombosis. • * Cerebrovascular disease (stroke). • * Thrombocytopenia. • * Pregnancy loss: • 1- There may be a history of recurrent fetal loss at any gestation. • 2- Late loss of a morphologically normal fetus is usually due to placental infarction and should also lead to tests for APS. • * Pulmonary embolism, pulmonary hypertension. • * Livedo reticularis (persistent red or blue pattern of the skin of trunk, arms or legs; it does not disappear on warming and may consist of regular broken or unbroken circles). • * Myocardial infarction. • * Retinal thrombosis.
Cutaneous manifestations. The aPL antibody is associated with many cutaneous conditions, including livedo reticularis , superficial thrombophlebitis , cutaneous necrosis, digital ischemia, and gangrene , stasis ulcers of the ankles , epidermal atrophy, splinter hemorrhages of the nailbeds , non-necrotizing purpura, and blue-toe syndrome. The aPL antibody may also be seen in patients with leukocytoclastic angiitis. Livedo reticularis may be part of Sneddon's syndrome, the other components of which include recurrent arterial or venous thrombosis, valvular abnormalities, stroke, and essential hypertension. The aPL antibody syndrome has also been found in patients with Dego's syndrome, a diffuse coagulopathy characterized by cutaneous necrosis and epidermal atrophy. It seems that skin lesions are an obvious external manifestation of a sometimes-insidious disease, are valuable markers for the syndrome. Skin biopsy, which can document vasculopathic potential in patients with aPL, may, therefore, be helpful. Livedo reticularis in young woman with APS.
Hughes Syndrome Diagnosis:Livedo reticularis" - the characteristic mottled appearance of skin seen in many patients with Hughes' Syndrome ( anti-phospholipid syndrome) Anti –phospholipid syndrome
Livedo reticularis of the upper extremities, which developed as petechiae in the classic lacy, reticular pattern and evolved as a confluent, non blanching, slightly raised purpuric rash in the same reticular pattern.
Antiphospholipid antibody syndrome in a patient with positive test results for antiphospholipid antibody and lupus anticoagulant who has systemic lupus erythematosus (SLE) and thrombocytopenia. Livedo reticularis of the upper extremities, which developed as petechiae in the classic lacy, reticular pattern, is observed
Livedo reticularis of the upper and lower extremities in a 15-year-old adolescent with primary antiphospholipid antibody syndrome. The pattern is lacy, flat, and nonblanching. The purplish hue is from stasis in the small vessel beds.
Common skin manifestations which may be present with APS include livedo reticularis , purpura and skin ulceration , and skin necrosis.
Palmar livedo reticularis associated with antiphospholipid antibody syndrome may range from a lacy, flat, reticulated pattern to a more confluent, non -blanching, slightly raised rash (secondary to extravasation of RBCs and plasma).
Primary or idiopathic LR (Livedo reticularis):LR without the presence of underlying disease is thought to be caused by spontaneous arteriolar vasospasm, which decreases oxygenated blood inflow, causing tissue hypoxia and increased deoxygenationof venous blood.SIGN VALUE:Despite the many potential causes, LR is still a valuable sign. Primary or idiopathic LR is a diagnosis ofexclusion and other causes should be ruled out first.• LR(livedo reticularis) has been shown to have a significant relationship with anti-phospholipid syndrome in the absence of SLE, with up to 40% of patients having LR as the first sign of the underlying prothrombotic disorder.• LR in a patient with SLE has been shown to be a significant predictor of the development of neuropsychiatric symptoms of SLE. A macular, bluish/purple discolouration of the skin that has a net- or lace-likeappearance.CAUSES:• Primary or idiopathic livedo reticularis (LR)• Elderly people• Secondary LR• Hypercoagulable/haematological states• Antiphospholipid syndrome• Snedden’s syndrome• Cryoglobulinaemia• Multiple myeloma• Polycythaemia• DVT• TTP• Vasculitis• Connective tissue disorders (e.g. SLE, Sjögren’s)• Embolisation (e.g. cholesterol embolisation syndrome)• Vessel wall deposition (e.g. calciphylaxis)• Amantadine adverse effect• Quinine adverse Livedo reticularis
Superficial phlebitis in young woman with associated axillary venous thrombosis and aPL.
Digital ischemia in patient with positive IgG aCL (anticardiolipin antibodies), VDRL, and intracardiac clot.
Stasis ulcer in 55-year-old patient with APS and venous thrombosis in lower extremity.
Acral purpura and ulceration of anti-phospholipid antibody syndrome
Antiphospholipid syndrome (APS), also known as 'sticky blood,' is an autoimmune disorder -- the result of the immune system essentially turning on the body and attacking it in error. In the case of APS, the body makes antibodies to its own blood proteins. Antiphospholipid syndrome can occur in individuals without any associated disease. This is called primary APS. The disorder may also occur with systemic lupus erythematosis (SLE) or another autoimmune disorder. This is called secondary APS. Antiphospholipid Syndrome
Primary anetoderma (PA) is a rare elastolytic disorder. PA occurs in normal skin idiopathically or after a systemic inflammatory process. Secondary anetoderma occurs after a skin inflammatory condition. Usually, PA is located on the trunk, shoulders, upper arms, and thighs. PA lesions manifest as a variable number of erythematous or skin-colored lesions that form either out-pouching or depressed areas of wrinkled skin. PA has also been associated autoimmunity such as SLE, discoid lupus erythematosus, lupus profundus, alopecia areata, vitiligo, hypothyroidism, multiple sclerosis, and Addison's disease . In PA, the predominant histopathologic finding is consistent with loss of elastic tissue in the reticular dermis and the occasional loss of elastic tissue in the papillary dermis, with or without a lymphohistiocytic infiltrate composed of neutrophils and other inflammatory cells , Several authors reinforced the association of PA as a cutaneous sign of APS, or as part of primary APS or secondary APS. Although not a specific marker of livedo reticularis for APS, it is recommended patients presenting with lesions consistent with anetoderma be screened for antiphospholipid antibodies as part of the evaluation of associated autoimmune disorders. Anetoderma and Antiphospholipid Syndrome
Splinter hemorrhages in 48-year-old female with cardiac mass, stroke, and positive aCL ( anticardiolipin antibodies).
Splinter Hemorrhage: In a patient with scleroderma. This is a nonspecific finding and can be associated with subacute bacterial endocarditis, SLE, rheumatoid arthritis, antiphospholipid syndrome, and trauma
Linear splinter hemorrhages are found under the nails of fingers and toes. These may be solitary or multiple and appear intermittently Splinter Hemorrhage
Antiphospholipid Antibody (Hughes') Syndrome: This syndrome is characterized by recurrent arterial or venous thrombotic events, such as in the fingers of this woman. It is associated with elevated titers of antiphospholipid antibodies such as lupus anticoagulant and anticardiolipin antibodies.
Digital infarctions in a patient with systemic lupus erythematosus with antiphospholipid syndrome (APS) and long-standing Raynaud symptoms. Multiple and repeated digital infarctions are depicted, resulting in ulcerations and scarring. Scars and hyperpigmentation are also seen on the palmer aspect of hands and fingers. Antiphospholipid syndrome
A patient with multisystem small vessel coagulopathy (microangiopathy) but no known underlying disease process. Extensive involvement of all digits is noted, some with distal infarction and dry gangrene, others healing with residual eschar (and undermining epithelialization), and some with re-epithelialization and scarring. Healed superficial epidermal damage and desquamation is also present. Antiphospholipid syndrome
A patient with multisystem small vessel coagulopathy (microangiopathy) but no known underlying disease process. Eschar is still present on first digit bilaterally. More superficial lesions are shown here, with evolution and healing of lesions on all other toes. Antiphospholipid syndrome
Antiphospholipid syndrome Actas Dermosifiliogr. 2012;103:832 103
Catastrophic Antiphospholipid Syndrome, i.e. Clotting Gone Wild!!
The presence of antiphospholipid antibodies in patients with APS and those who are aPL positive can increase the risk of developing a thrombosis (blood clot) in a vein or artery,. Without treatment, patients often experience repeated clots which can disturb blood flow to important organs, impairing their ability to function.
thrombosis in the dermis of the skin in this patient with antiphospholipid syndrome .Skin biopsy is usually necessary for a differential diagnosis. Absence of vasculitis and the finding of non-inflammatory thrombosis of small dermal and hipodermal arteries and veins are the characteristic cutaneous lesions of antiphospholipid syndrome.
Organizing thrombus in an aortic valve in a patient with positive test results for antiphospholipid antibody and lupus anticoagulant who has systemic lupus erythematosus (SLE) and recurrent thrombotic events
Trichrome stain of a thrombus in the intestinal serosa in a patient who has positive test results for antiphospholipid antibody and lupus anticoagulant and who has systemic lupus erythematosus (SLE) and catastrophic antiphospholipid antibody syndrome (CAPS).
Analogy between AMR and antibody-mediated pregnancy loss. In this scheme the analogy between antibody-mediated rejection of a transplanted graft and 'antibody-mediated pregnancy loss' is schematically shown. HLA, human lymphocyte antigen.
Anti-Phospholipid Antibody • What happens most frequently in APS is blood clotting. Pregnancies are lost because blood clots form in the placenta and starve the baby of nutrition. Treatment is the use of anticoagulation. In pregnancy, heparin is used. This gives the fetus an 80-90% chance of survival, a drastic improvement from the 1980's when fetal survival was around 20%. • However, pregnancies are not normal. Normal pregnancy is 40 weeks. In APS, it is more common to deliver the baby between 30-35 weeks, and between 3-4 pounds. Heparin protects placenta partially, but not fully so that the baby gets enough nutrition to survive longer in the mother. Once born, the babies do fine. • Treatment for people who clot is to also use anticoagulation. There are more options available in this case. Warfarin (Coumadin) can be used with blood clots. This medication is commonly used for people with strokes and coronaries. It is used differently in use of patients with APS. People with APS must take a very high dose; moderate doses do not work well. The goal is to get people who are at the threshold of danger, which is a 10% risk every year for having a hemorrhage. Reaching this level of anticoagulation can virtually prevent any new clotting. Sometimes aspirin is used, but this is only partially effective. • Another treatment is an experimental therapy called IV immunoglobulin