Download
1 / 54
550 likes | 607 Views
Explore the intricate mechanisms of renovascular hypertension involving the renal system, sodium, and the renin-angiotensin system. Learn about physiological stimulation of renin release, angiotensin peptides, receptor subtypes, and antihypertensive agents.

E N D
Kidney, Sodium, Renin-Angiotensin System Renovascular Hypertension Andreas Pittaras MD
Renin protein in the juxtaglomerular cells of the afferent arteriole
Major mechanisms governing renin release • Individual nephron signals • Low macula densa sodium chloride (stimulates) • Decreased afferent arteriolar pressure (stimulates) • Whole kidney modulating signals • Angiotensin II negative feedback (inhibits) • β-1 receptor stimulation (stimulates) • Other humoral factors Vasopressin (inhibits) • Atrial natriuretic peptide (inhibits) • Dopamine DA-1 receptor (stimulates) • Local effectors • Prostaglandins (stimulate) • Nitric oxide (inhibits) • Adenosine (inhibits) • Kinins (stimulate)
Physiologic stimulation of renin release PHYSIOLOGYPHARMACOLOGY Blood pressureAntihypertensive agents Fluid volumeStimulators Sodium intakeRenin-angiotensin blockade HydrationDiuretics DiureticsVasodilators Menstrual cycleSuppressors Diurnal changesβ-Adrenergic blockers PostureCentral α2-adrenergic agonists Potassium intakeNeutral Protein intakeCalcium antagonists
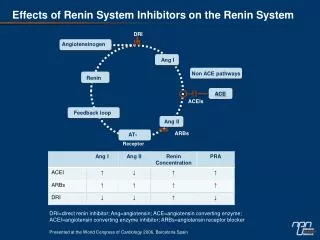
Half-life of renin and angiotensin Metabolism of the renin-angiotensin system COMPONENTHALF-LIFE IN CIRCULATIONDEGRADING ENZYME(S) Renin15 -20 min - Angiotensinogen4 -16 HRenin Angiotensin I1 -2 minAngiotensin-converting enzyme Angiotensin IISecondsAminopeptidase A, Εndopeptidase, Ρrolylcarboxypeptidase
Angiotensin peptides and receptor subtypes that interact with each peptide RECEPTORANGIOTENSIN NoneAngiotensinogen Asp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-Leu-Val-Ile-His-Asn-Glu Renin NoneAngiotensin I NH2-Asp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-Leu-COOH Angiotensin-converting enzyme AT1, AT2Angiotensin II Asp-Arg-Val-Tyr-Ile-His-Pro-Phe Angiotensinases AT1, AT2Angiotensin III Arg-Val-Tyr-Ile-His-Pro-Phe Angiotensinases UnknownAngiotensin (1-7) Asp-Arg-Val-Tyr-Ile-His-Pro Angiotensinases AT4Angiotensin (3-7) Val-Tyr-Ile-His-Pro
Heterogeneity in the angiotensin II receptor population Classification criteria of angiotensin receptor subtypes AT1AT2 Potency orderAngiotensin II > angiotensin IIIAngiotensin II =angiotensin III Selective antagonistsILosartanPD 123177 (Parke-Davis, NJ) PD 123319 (Parke-Davis) ValsartanCGP 42112A (Novartis) Eprosartan Zorsartan Irbesartan Candesartan Telmisartan Tasosartan Effector pathwaysPhospholipase CGuanylate cyclase Phospholipase D Adenylate cyclase Sensitivity to dithiothreitol (sulfhydryl-reducing agents)BindingBinding AffinityNo change Effect of GppNHpHill coefficient to no Change ~1
Renal effects of angiotensin subtype-2 receptor • Release of bradykinin, nitric oxide, and cGMP • Cell differentiation • Antiproliferation • Apoptosis • Vasodilation
Renal effects of angiotensin II • Decreased renal blood flow • Proportionately increased efferent arteriolar resistanceincreased glomerular capillary hydrostatic pressure increased filtration • Glomerular mesangial cell contraction decreased glomerular capillary surface area available for filtration decreased filtration (offsets above effect) • Decreased medullary blood flow • Increased tubular sodium reabsorption sodium retention
Causes of renal artery stenosis • Clinical clues suggesting renovascular hypertension • Systolic/diastolic epigastric, subcostal, or flank bruit • Accelerated or malignant hypertension (HTN) • Unilateral small kidney discovered by any clinical study • Severe HTN in child or young adult, or after age 50 y • Sudden development or worsening of HTN at any age • HTN and unexplained impairment of renal function • Sudden worsening of renal function in hypertensive patient • Hypertension refractory to appropriate three-drug regimen • Impairment in renal function in response to ACE inhibitor • Extensive occlusive disease in coronary, cerebral, and peripheral circulation
Diagnostic indicators for renovascular hypertension Diagnostic studies for renovascular hypertension • SENSITIVITY, %SPECIFICITY, % • Rapid sequence IVP7486 • Isotope renography 9395 • with ACE inhibitiontest • Peripheral vein PRA with 7489 • ACE inhibition test (captopril test) • Renal vein ratio of PRA test • (stenotic/contralateral): • >1.38540 • >1.97860 • Peripheral vein PRA9296 • Intravenous digital 8889 • subtraction angiography • Doppler ultrasonography8693 • MRI9795 • Renal artery angiography100100
The captopril test • Criteria for renovascular hypertension • Stimulated PRA of 12 ng/mL/h • Absolute increase in PRA of 10 ng/mL/h • Increase in plasma renin activity PRA of 150% or 400% if baseline PRA is <3 ng/mL/h
Objectives in the management of renovascular hypertension Outcome after angioplasty or surgery for renal artery stenosis ETIOLOGYATHEROMAFIBROMUSCULAR DYSPLASIA TreatmentAngioplastySurgeryAngioplastySurgery Patients3911310175486 BP response Cured19455064 ( 56- 81) Improved52294223 ( 5 -40) Failed3024911 ( 0 -25)
Selective renal arteriogram of a 43-year-old nonsmoking male