Download
1 / 17
170 likes | 386 Views
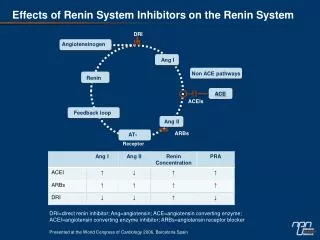
Inhibitors of the Renin-Angiotensin System in Hypertension Therapy. Dr. Thomas Abraham PHAR 417: Fall 2004. The Renin-Angiotensin System in hypertension. Ø Approximately 20% of pts. with essential hypertension have high plasma renin activity while another 20% have low renin activity.

E N D
Inhibitors of the Renin-Angiotensin System in Hypertension Therapy Dr. Thomas Abraham PHAR 417: Fall 2004
The Renin-Angiotensin System in hypertension • ØApproximately 20% of pts. with essential hypertension have high plasma renin activity while another 20% have low renin activity. • A significant role for the renin-angiotensin system in hypertension appears probable and high renin pts. respond well to ACE inhibitors and angiotensin II receptor antagonists.
The Renin-Angiotensin System in hypertension Factors that promote renin release: 1. Amount of NaCl in the glomerular filtrate ØMacula densa cells on the wall of the thick ascending loop of Henle detect decreased NaCl in the filtrate and trigger the juxtaglomerular cells to release renin into the afferent arteriole. • Increased NaCl in filtrate increases NaCl transport into the macula densa cells which release adenosine to signal Juxtaglomerular cells to decrease renin release. • Decreased NaCl transport into macula densa cells results in release of PGI2 which increases renin release by the JG cells.
The Renin-Angiotensin System in hypertension • Factors that promote renin release: (Cont.) • 2. Intrarenal baroreceptors • ØRenin release is also influenced by intrarenal baroreceptors that detect low pressure in the afferent arterioles. • 3. Sympathetic nervous system activity • Enhanced sympathetic nerve activity results in NE release which stimulates b1-adrenoceptors on JG cells to cause renin secretion.
The Renin-Angiotensin System in hypertension Factors Promoting Renin Release by the Juxtaglomerular cells
The Renin-Angiotensin System in hypertension • Factors that decrease renin release: • Circulating angiotensin II activates AT1 receptors on JG cells to decrease renin release • Vasoconstriction by angiotensin II increases systemic blood pressure to decrease renin release by: • - Decreasing sympathetic tone to the JG cells • - Constricting afferent arterioles • - Decreasing Na reabsorption in the proximal tubules
The Renin-Angiotensin System in hypertension Consequences of Plasma Renin and ACE actions
The Renin-Angiotensin System in hypertension • Physiological Roles of Angiotensin II: • Direct vasoconstrictor of various vascular beds to increase TPR • Enhanced NE release from sympathetic nerve endings • Blunts the baroreceptor-mediated decrease in sympathetic nerve activity • Releases catecholamines from adrenal medulla • Stimulates aldosterone release from adrenal cortex • Increase/decrease GFR by constriction of efferent/afferent arterioles
The Renin-Angiotensin System in hypertension Angiotensin II receptors: Angiotensin II via the AT1 receptor produces Phosphoinositide hydrolysis in vascular smooth muscle cells to cause smooth muscle contraction and increased PVR Majority of the physiological effects of angiotensin II is due to the function of the AT1 receptor. The AT2 receptor may have additional roles in embryological development and also regulate apoptosis, decrease cell proliferation and vasodilation AT1
The Renin-Angiotensin System in hypertension • Role of renin-angiotensin system in cardiovascular pathology: • Increased angiotensinogen levels are associated with essential hypertension • Elevated serum ACE levels may be associated with increased risk of cardiac ischemia, coronary artery spasm, left ventricular hypertrophy and hypertension • Polymorphisms of the AT1 receptor may be associated with hypertension, hypertrophic cardiomyopathy, aortic stiffness
The Renin-Angiotensin System in hypertension Angiotensin-Converting Enzyme Inhibitors in Hypertension Therapy ØACE inhibitors were first isolated from pit viper venom in the 1960s and shown to increase bradykinin levels and decrease angiotensin II blood levels to cause decreases in blood pressure. ØACE inhibitors decrease circulating levels of angiotensin II and may also increase levels of bradykinin (a potent vasodilator) to produce antihypertensive effects.
The Renin-Angiotensin System in hypertension • ØAll the ACE inhibitors except captopril, enalaprilat and lisinopril are ester prodrugs that have to be converted to the active carboxylic acid derivative. All these agents have oral bioavailability and all except fosinopril and spirapril are primarily eliminated by the kidneys. • benazapril, enalapril, perindopril, quinapril, ramipril, trandolapril, moexipril • ØACE inhibitors decrease PVR without affecting cardiac output or causing baroreceptor reflex increase in sympathetic activity to the heart. • Lack of baroreflex may be due to resetting of the baroreceptors to a lower point or blunting sensitivity. • Generally hypertensive pts. show greater lowering of BP than normotensive subjects and high renin hypertensives are most susceptible to the effects of these drugs.
The Renin-Angiotensin System in hypertension • ØPrimary therapeutic uses of ACE inhibitors: hypertension, congestive heart failure, diabetic nephropathy, and post-myocardial infaction. • ØAdverse effects include: severe first dose hypotension (esp. in hypovolemic pts, high renin pts.), acute renal failure, hyperkalemia, dry cough, wheezing and angioedema. Other effects observed are altered taste, skin rash and drug fever. These agents are contraindicated in the 2nd and 3rd trimesters due risk of fetal hypotension, anuria, renal failure and developmental malformations. • ØDrug interactions include: hyperkalemia with K+-supplements or K+-sparing diuretics; NSAIDS decrease hypotensive effects by blocking bradykinin-mediated prostaglandin formation.
The Renin-Angiotensin System in hypertension Angiotensin Receptor Antagonists ØThese agents appear to be competitive antagonists (e.g. losartan, eprosartan, candesartan, irbesartan) but most seem to dissociate very slowly from the receptor (candesartan, EXP 3174). Potency order for the AT1 receptor: candesartan> irbesartan> telmisartan = valsartan = EXP3174> losartan
The Renin-Angiotensin System in hypertension • ØThese agents are selective for the AT1 receptor with poor affinity for the AT2 receptor. • These antagonists decrease angiotensin II-mediated: vasoconstriction, enhanced NE release at sympathetic nerve endings, increased catecholamines release from the adrenals, increased aldosterone synthesis and release. • May indirectly activate AT2 receptors by blocking AT1 receptors and causing elevated Angiotensin II levels • These agents may also have beneficial effects on limiting smooth and cardiac muscle hypertrophy seen in hypertension and heart failure. • As with the ACE inhibitors BP is reduced without altering cardiac output • Does not interfere with bradykinin metabolism
The Renin-Angiotensin System in hypertension • ØGenerally these agents show poor to modest oral bioavailability (<50%) except for irbesartan (~70%) and tend to be highly bound to plasma proteins. • Most of them undergo extensive hepatic metabolism to active and inactive metabolites. Elimination of metabolites may be via renal or hepatic route. Doses of losartan and valsartan need to be reduced in liver failure. • Candesartan, irbesartan, eprosartan require renal and hepatic elimination. Losartan, telmisartan, valsartan have mostly hepatic elimination.
The Renin-Angiotensin System in hypertension • ØPrimary adverse effects: • first dose hypotension • acute renal failure and hyperkalemia are common to ACEI as well • risk to developing fetus prevents its use in pregnancy • dry cough and angioedema seen with ACEIs is not seen with AT1 antagonists probably because those affects are due to potentiation of bradykinin effects following kininnase inhibition.