Download
1 / 22
260 likes | 601 Views
Human Immunodeficiency Virus (HIV). Andrew Borst Isabel VanDerslice Image: http://www.npr.org/blogs/pictureshow/2011/02/22/133868260/sciviz. A World Pandemic. HIV has enormous social, economic and humanitarian implications

E N D
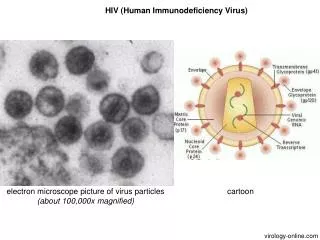
Human Immunodeficiency Virus (HIV) Andrew Borst Isabel VanDerslice Image: http://www.npr.org/blogs/pictureshow/2011/02/22/133868260/sciviz
A World Pandemic HIV has enormous social, economic and humanitarian implications HIV and AIDS is decimating populations, taxing health infrastructures, and crippling economies, and creating unsustainable population age distributions Some parts of Africa have a prevalence rate of 1 in 3. For many, infection is inevitable, and treatment beyond reach. From its discovery in 1981 to 2006, AIDS killed more than 25 million people.
The Spread of HIV Tip of the Day: Use condoms and clean needles! • Spread through sexual contact, intravenous drug use (infected blood), and mother-to-child during birthing and nursing. • Birthing transmittance rate is 15-30% for mothers infected with HIV. • To minimize risk, antiretroviral therapy is recommend prior to (for the mother) and after birth (for the baby). • Does not spread through mucous membranes, only blood contact. • HIV is a fragile virus
HIV-1 Binds to CCR5 co-receptor Most common strain of the Human Immunodeficiency Virus What most professionals refer to when they reference HIV HIV-2 Binds to CXCR4 co-receptor Uncommon; mostly found in Western Africa or individuals of whom are in the later phases of disease progression. HIV-1 and HIV-2 Higher HIV-2 prevalence-rates here
Vaccine and Treatment • It is difficult to make a vaccine for HIV due to several characteristics of the virus • HAART: Highly active anti-retroviral therapy is the only effective treatment, but resistance occurs, especially after many years of treatment. • Gene therapy appears to be a good candidate for future HIV treatment options.
Vaccine and Treatment Anti-retroviral therapy has significantly reduced the death toll associated with AIDS. It is difficult to make a vaccine for HIV due to several characteristics of the virus HAART: Highly active anti-retroviral therapy is the only effective treatment, but resistance occurs, especially after many years of treatment. Gene therapy appears to be a good candidate for future HIV treatment options.
Human hematopoietic stem/progenitor cells modified by zinc-finger nucleases targeted to CCR5 controls HIV-1 in vivo Nathalia Holt, Jianbin Wang, Kenneth Kim, Geoffrey Friedman, Xingchao Wang, Vanessa Taupin, Gay M Crooks, Donald B Kohn, Philip D Gregory, Michael C Holmes & Paula M Cannon
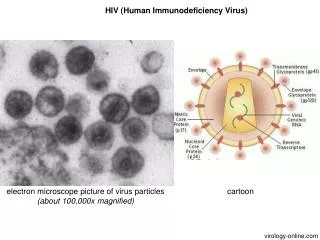
HIV-1 Infection Transmembrane proteins on the surface of the virus interact with receptors on the host cell Two interactions are needed for entry—CD4-gp120 and a chemokine coreceptor, usually CCR5. The main reservoirs for HIV in the body are wherever immune cells reside, such as the spleen and intestine. HIV is also found in the follicular dendritic cell (FDC) network. In tonsils and adenoids of HIV-infected patients, infected macrophages fuse into multinucleated giant cells that produce huge amounts of virus.
Co-receptor CCR5 Permits HIV-1 Entry • CCR5 is the major co-receptor used by HIV-1 and is expressed on key T-cell subsets and monocytes. • CCR5Δ32 is a relatively common allele in Western Europe • Confers an innate resistance to HIV-1 infection • CCR5 antagonists have proved to be an effective salvage therapy in patients infected with drug-resistant HIV-1 Kuby Immunology says CCR5 is only expressed on Monocytes, but this is an extremely misleading oversimplification.
ZFN-mediated disruption of CCR5 in CD34+ HSPCs. • ZFN: Zinc Finger Nuclease • Artificial restriction enzymes generated by fusing a zinc finger DNA-binding domain to a DNA-cleavage domain. • Cel 1 nuclease: • Preferentially cleaves DNA at distorted duplexes caused by mismatches. • Used for quantification of the CCR5 disrupted alleles. • NSD Mice: • NOD SCID IFγ-null Mice • Non-obese diabetic severe combined immunodeficiency interferon-gamma null mice. • Lack T, B, and NK cells • Deficient in multiple cytokine signaling pathways • Defects in innate immunity. Fun Fact: “Cel” in Cel 1 nuclease stands for celery! Image courtesy of Wikipedia: “The only website on the internet guaranteed to be 90% accurate!”
ZFN-mediated disruption of CCR5 in CD34+ HSPCs. Figure 1 Analysis a) Representative gel showing extent of CCR5 disruption in CD34+ HSPCs 24 hours after nucleofection Neg: No gene digestion Mock: No gene digestion ZFN: Gene digestion b) Mean percentage of human CD45+ cells in peripheral blood of mice 8 weeks after transplantation. No statistical difference between Neg, Mock, and ZFN groups. c) Fluorescence-activated cell sorting (FACS, or flow cytometry) profiles of human cells of various organs from one ZFN-treated mouse. Results indistinguishable from that of mice transplanted with unmodified cells. Holds true for both the location of cells and their frequency in that particular tissue.
Protection of human CD4+ T cells in peripheral blood of HIV-infected mice previously engrafted with ZFN-modified CD34+ HSPCs. Figure 2 Analysis a) FASC readouts showing human CD4+ and CD8+ T-cells in peripheral blood of representative animals from each of three cohorts. Uninfected: Normal CD4+ T-cell levels HIV-1 Infected (Negative): Complete T-cell depletion HIV-1 Infected (ZFN-treated): Normal CD4+ T-cells b) Ratio of human CD4+ to CD8+ lymphocytes in peripheral blood of individual mice to which were infected with HIV-1. Measured pre-infection and 6-8 weeks post-infection. Significant reduction in CD4+/CD8+ T-cell ratio in post-infection untreated mice.
Effects of HIV-1 infection on human cells in HSPC-engrafted NSG mice. Figure 3 Analysis a) FACS analysis of human cells in tissues of representative NSG mice from three cohorts. SSC means “side scatter” of light. Bone Marrow: No CD45 cell loss Not a major organ for HIV-1 infection Spleen: Reduction of CD4+ T-helper cells post HIV-1 infection w/o ZFN treatment. Thymus: Completeloss of CD4+ and CD8+ T-cells. Small intestine: Complete loss of all human lymphocytes w/o ZFN treatment. b) Immunohistochemical analysis of human CD3 expression in small intestine, and CD4 expression in spleen of representative mice.
Reasons for CD4+ and CD8+ T-cell Depletion in the Thymus Proposed to occur as a consequence of the upregulation of CCR5 on these cells during HIV-1 infection. Explains observed reduction of both of these cell types in the thymus and other tissues. Image: M. Germana Paterlini (2002). Structural modeling of the Chemokine Receptor CCR5: Implications for Ligand Binding and Selectivity. Biophysical Journal 3012-3031
HIV-1 infection selects for disrupted CCR5 alleles. Figure 4 Analysis a) Mean +- s.d. levels of CCR5 disruption in sequential peripheral blood samples taken from mice. b) Mean +- s.d. levels of CCR5 disruption in necropsied mice 12-weeks post-infection or with uninfected ZFN-treated cohorts. Gel shows increased levels of digestion products in infected mice indicating increased CCR5-/- cell selection. c) Contour FACS analysis of human CD4+ T-cells in small intestine and spleen of one representative animal from each cohort. Expected results were expected. d) Mean +- s.d. numbers of human CD4+ cells and CD4+CCR5+ per 5,000 cells analyzed from different sections of the intestine. S = small intestine L = large intestine E = intraepithelial lymphocytes P = lamina propria lymphocytes
ZFN activity produces heterogeneous mutations in CCR5. Figure 5 Analysis Mutations observed in ZFN-treated mice cohorts. WT Deletions Insertions
Control of HIV-1 replication in mice receiving ZFN -treated CD34+ HSPCs Figure 6 Analysis a) Mean +- s.d. levels of HIV-1 RNA and percent CD4+ T-cells in peripheral blood. HIV-1 RNA levels in non-ZFN-treated cohorts increase post-infection, but drop off after 6 weeks. Reduction in CD4+ cells limits viral reproducibility. T-cell levels remain mostly constant in ZFN-treated mice barring initial deletion of residual CD4+CCR5+ T-cells. b) Mean +- s.d. levels of HIV-1 RNA in small and large intestine lamina propria from 8 and 12 week necropsied mice. Significantly less HIV-1 in ZFN-treated mice.
Control of HIV-1 replication in mice receiving ZFN -treated CD34+ HSPCs
Conclusions • Findings suggest that transplantation of HSPCs modified by CCR5-specific ZFNs may provide permanent supply of HIV-resistant progeny. • ZFN also modified CCR2; nonspecific cleavage must be evaluated in larger future studies. • Scientific rational for CCR5 modification stems from HIV+ Leukemia patient being effectively cured of his infection. • Immune hyperactivation suppressed with CCR5-/- mutants. • Immune hyperactivation underlies much of the pathology of AIDS. • This approach could be considered a “one-shot” treatment option. • Procedures for autogenic or allogeneic transplantation already established. • Targeting CCR5 may promote CXCR4-tropic HIV development. • Not observed in patients unless virus was present prior to treatment. • Could be used as a backup therapy, or done in addition to HAART.
A quick word about using proper grammar “PCR reaction” = BAD “HIV virus” = The WORST “Isabel and I’s paper” = The reason for this slide. Now…any questions?