Download
1 / 14
160 likes | 390 Views
DENGUE FEVER UPDATE. 30/3/2014. Background . Dengue fever is a severe, flu-like illness that affects infants, young children and adults, but seldom causes death .

E N D
DENGUE FEVER UPDATE 30/3/2014
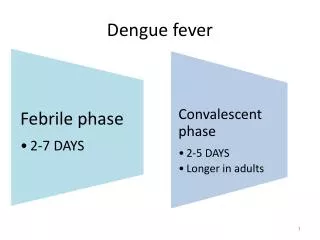
Background • Dengue fever is a severe, flu-like illness that affects infants, young children and adults, but seldom causes death. • Dengue is transmitted by the bite of a mosquito infected with one of the four dengue virus serotypes. It is a febrile illness that affects infants, young children and adults with symptoms appearing 3-14 days after the infective bite. • Dengue is not transmitted directly from person-to-person and symptoms range from mild fever, to incapacitating high fever, with severe headache, pain behind the eyes, muscle and joint pain, and rash. • There is no vaccine or any specific medicine to treat dengue. People who have dengue fever should rest, drink plenty of fluids and reduce the fever using paracetamol or see a doctor. • Severe dengue (also known as dengue hemorrhagic fever) is characterized by fever, abdominal pain, persistent vomiting, bleeding and breathing difficulty and is a potentially lethal complication, affecting mainly children. • Early clinical diagnosis and careful clinical management by trained physicians and nurses increase survival of patients.
Global burden • The incidence of dengue has grown dramatically around the world in recent decades. Over 2.5 billion people – over 40% of the world's population – are now at risk from dengue. WHO currently estimates there may be 50–100 million dengue infections worldwide every year. • Before 1970, only nine countries had experienced severe dengue epidemics. The disease is now endemic in more than 100 countries in Africa, the Americas, the Eastern Mediterranean, South-east Asia and the Western Pacific. The American, South-east Asia and the Western Pacific regions are the most seriously affected. • Cases across the Americas, South-east Asia and Western Pacific have exceeded 1.2 million cases in 2008 and over 2.3 million in 2010 (based on official data submitted by Member States). • Recently the number of reported cases has continued to increase. In 2013, 2.35 million cases of dengue were reported in the Americas alone, of which 37 687 cases were severe dengue.
Global burden ( increasing threat) • Not only is the number of cases increasing as the disease spreads to new areas, but explosive outbreaks are occurring. The threat of a possible outbreak of dengue fever now exists in Europe and local transmission of dengue was reported for the first time in France and Croatia in 2010 and imported cases were detected in three other European countries. • In 2012, an outbreak of dengue on Madeira islands of Portugal resulted in over 2000 cases and imported cases were detected in 10 other countries in Europe apart from mainland Portugal. • In 2013, cases have occurred in Florida (United States of America) and Yunnan province of China. • Dengue also continues to affect several south American countries notably Honduras, Costa Rica and Mexico. In Asia, Singapore has reported an increase in cases after a lapse of several years and outbreaks have also been reported in Laos. • In 2014, trends indicate increases in the number of cases in the Cook Islands, Malaysia, Fiji and Vanuatu, with Dengue Type 3 (DEN 3) affecting the Pacific Island countries after a lapse of over 10 years. • An estimated 500 000 people with severe dengue require hospitalization each year, a large proportion of whom are children. About 2.5% of those affected die.
Transmission • The Aedesaegypti mosquito is the primary vector of dengue. The virus is transmitted to humans through the bites of infected female mosquitoes. After virus incubation for 4–10 days, an infected mosquito is capable of transmitting the virus for the rest of its life. • Infected humans are the main carriers and multipliers of the virus, serving as a source of the virus for uninfected mosquitoes. Patients who are already infected with the dengue virus can transmit the infection (for 4–5 days; maximum 12) via Aedes mosquitoes after their first symptoms appear. • The Aedesaegypti mosquito lives in urban habitats and breeds mostly in man-made containers. Unlike other mosquitoes Ae. aegypti is a daytime feeder; its peak biting periods are early in the morning and in the evening before dusk. • Female Ae. aegypti bites multiple people during each feeding period.
Current Country Status • The total positives so far is 144 with one death in January 2014 outbreak • (June 2010 40 cases in DSM, May – July 2013 172 cases confirmed in DSM) • Established surveillance sites in the three municipality for all patients presenting with fever : Temeke – 4 sites, Ilala- 5 sites , Kinondoni- 5 site ( IST volunteers to send samples) , TPDF 5 sites • Vector Control : through CBO/ CORPs environmental clearing of breeding sites & Fogging in Temeke, Kinondoni municipalities • Risk communication : radio spots and TV , (WB support) • Laboratory confirmation: lab Tech & H/W orientations on sample collection and testing, conducted under CDC support • World Health day 2014 focus on Vector borne Diseases including Dengue fever – Joint Press release on 6 April 2014 ( MOHSW & WHO)
Surveillance: Follow up on proper adherence to Std case definition and SOPs • Routine surveillance • Target: All patients until outbreak is declared over • Record all cases that fit in SCD in the register • items in the register, Name, Age, Place of Residence, Symptoms, Diagnosis, Treatment • Sentinel surveillance • Mwananyamala under Italian support • When to report • Weekly IDWE reports
Laboratory • WCO supported extraction kits procurement • CDC supported TOT lab technicians training • NHQAL conducted training to 2 lab technicians and 1 clinician (3@HF) from all HFs in the surveillance area. • Request for Dengue RDT procured, AFRO technical guidance • Lab needed more blood collection tubes for surveillance purposes - procured.
Risk communication • 5 weeks 3 slots / day in TV & Radio – support from WB of TZS 7 Million • UNICEF assisted printing of IEC materials • Media orientation on VHF & Dengue fever supported by WCO ( one day workshop) facilitation was by WCO & MOHSW – Epidemiology unit • MOHSW required to monitor the impact
Municipals • Public mobilization and sensitization on destroying breeding sites ( use of mega phones) by CBOs/ CORPS • Adherence to sample collection manual • Proper documentation in surveillance registers • Daily collection of status report and feed back received from laboratory • Coordination of other vector control measures including fogging
Other initiatives: • TPDF joined the efforts in surveillance through their army/ camp hospitals • COSTECH work with NIMR support to vector studies and other surveillance activities (TZS 31 ML) • Involvement of Private Hospital Association to increase PPP in surveillance as many people also attend private hospitals
Key challenges • Report sharing and feedback at all levels • Sample transportation to National lab • Supportive supervision to HFs • RDTs- sensitivity ! Dengue fever VS MOHSW decision in order to reduce PCR testing ! • Impact of TV & Radio spot- Monitoring by MOHSW • Laboratory results feed back to Municipal FP • Laboratory supplies to sentinel surveillance sites: Blood collection tubes • Surveillance in other regions. • Establishment of a strong Vector Borne disease unit under environmental health section
Future Actions Planned • Development of Viral Hemorrhagic Fever (VHF) control strategy 2014 – 2018 ( will include dengue fever) • Strengthen public awareness through IEC materials and TV/ radio spots