Download
1 / 1
10 likes | 180 Views
Orientation and Mobility Training Service for the Blind under the Universal Health Coverage Program in Thailand. THE WORLD REPORT ON DISABILITY: IMPLICATIONS FOR ASIA AND THE PACIFIC. 5-7 December 2011 Sydney, Australia. Please insert the document ID here: D0xxp.

E N D
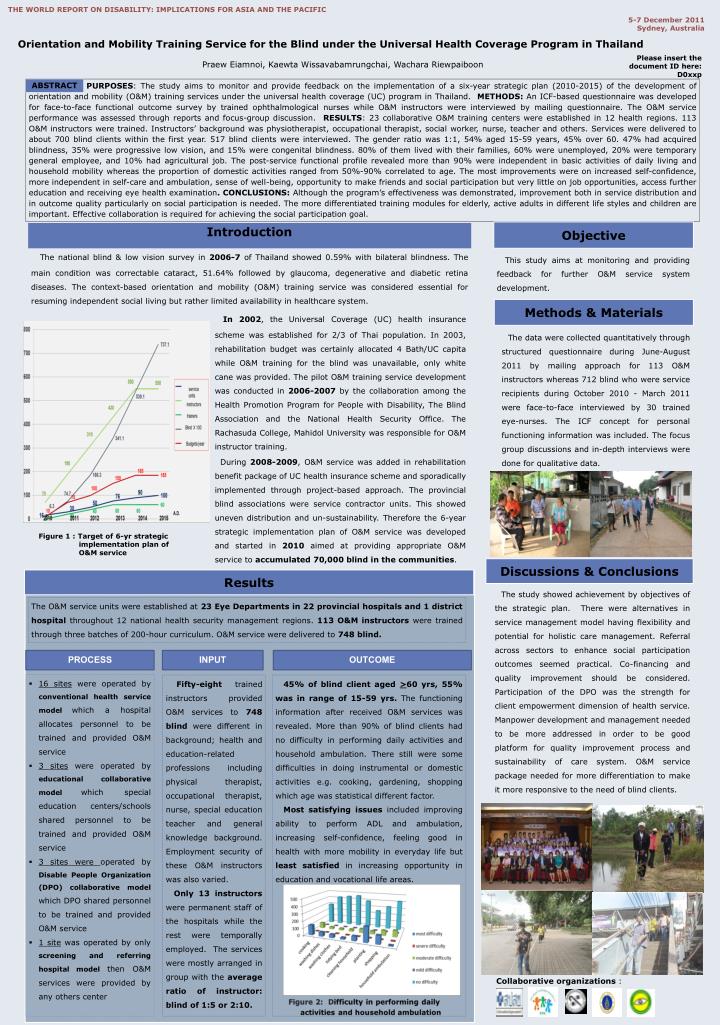
Orientation and Mobility Training Service for the Blind under the Universal Health Coverage Program in Thailand THE WORLD REPORT ON DISABILITY: IMPLICATIONS FOR ASIA AND THE PACIFIC 5-7 December 2011Sydney, Australia Please insert the document ID here: D0xxp Praew Eiamnoi, Kaewta Wissavabamrungchai, Wachara Riewpaiboon PURPOSES: The study aims to monitor and provide feedback on the implementation of a six-year strategic plan (2010-2015) of the development of orientation and mobility (O&M) training services under the universal health coverage (UC) program in Thailand. METHODS: An ICF-based questionnaire was developed for face-to-face functional outcome survey by trained ophthalmological nurses while O&M instructors were interviewed by mailing questionnaire. The O&M service performance was assessed through reports and focus-group discussion. RESULTS: 23 collaborative O&M training centers were established in 12 health regions. 113 O&M instructors were trained. Instructors’ background was physiotherapist, occupational therapist, social worker, nurse, teacher and others. Services were delivered to about 700 blind clients within the first year. 517 blind clients were interviewed. The gender ratio was 1:1, 54% aged 15-59 years, 45% over 60. 47% had acquired blindness, 35% were progressive low vision, and 15% were congenital blindness. 80% of them lived with their families, 60% were unemployed, 20% were temporary general employee, and 10% had agricultural job. The post-service functional profile revealed more than 90% were independent in basic activities of daily living and household mobility whereas the proportion of domestic activities ranged from 50%-90% correlated to age. The most improvements were on increased self-confidence, more independent in self-care and ambulation, sense of well-being, opportunity to make friends and social participation but very little on job opportunities, access further education and receiving eye health examination. CONCLUSIONS: Although the program’s effectiveness was demonstrated, improvement both in service distribution and in outcome quality particularly on social participation is needed. The more differentiated training modules for elderly, active adults in different life styles and children are important. Effective collaboration is required for achieving the social participation goal. ABSTRACT Objective Introduction The national blind & low vision survey in 2006-7 of Thailand showed 0.59% with bilateral blindness. The main condition was correctable cataract, 51.64% followed by glaucoma, degenerative and diabetic retina diseases. The context-based orientation and mobility (O&M) training service was considered essential for resuming independent social living but rather limited availability in healthcare system. This study aims at monitoring and providing feedback for further O&M service system development. Methods & Materials In 2002, the Universal Coverage (UC) health insurance scheme was established for 2/3 of Thai population. In 2003, rehabilitation budget was certainly allocated 4 Bath/UC capita while O&M training for the blind was unavailable, only white cane was provided. The pilot O&M training service development was conducted in 2006-2007 by the collaboration among the Health Promotion Program for People with Disability, The Blind Association and the National Health Security Office. The Rachasuda College, Mahidol University was responsible for O&M instructor training. The data were collected quantitatively through structured questionnaire during June-August 2011 by mailing approach for 113 O&M instructors whereas 712 blind who were service recipients during October 2010 - March 2011 were face-to-face interviewed by 30 trained eye-nurses. The ICF concept for personal functioning information was included. The focus group discussions and in-depth interviews were done for qualitative data. During 2008-2009, O&M service was added in rehabilitation benefit package of UC health insurance scheme and sporadically implemented through project-based approach. The provincial blind associations were service contractor units. This showed uneven distribution and un-sustainability. Therefore the 6-year strategic implementation plan of O&M service was developed and started in 2010 aimed at providing appropriate O&M service to accumulated 70,000 blind in the communities. Figure 1 : Target of 6-yr strategic implementation plan of O&M service Discussions & Conclusions Results • The study showed achievement by objectives of the strategic plan. There were alternatives in service management model having flexibility and potential for holistic care management. Referral across sectors to enhance social participation outcomes seemed practical. Co-financing and quality improvement should be considered. Participation of the DPO was the strength for client empowerment dimension of health service. Manpower development and management needed to be more addressed in order to be good platform for quality improvement process and sustainability of care system. O&M service package needed for more differentiation to make it more responsive to the need of blind clients. The O&M service units were established at 23 Eye Departments in 22 provincial hospitals and 1 district hospital throughout 12 national health security management regions. 113 O&M instructors were trained through three batches of 200-hour curriculum. O&M service were delivered to 748 blind. PROCESS INPUT OUTCOME • 16 sites were operated by conventional health service modelwhich a hospital allocates personnel to be trained and provided O&M service • 3 sites were operated by educational collaborative modelwhich special education centers/schools shared personnel to be trained and provided O&M service • 3 sites were operated by Disable People Organization (DPO) collaborative modelwhich DPO shared personnel to be trained and provided O&M service • 1 site was operated by only screening and referring hospital modelthen O&M services were provided by any others center Fifty-eight trained instructors provided O&M services to 748blind were different in background; health and education-related professions including physical therapist, occupational therapist, nurse, special education teacher and general knowledge background. Employment security of these O&M instructors was also varied. Only 13 instructors were permanent staff of the hospitals while the rest were temporally employed. The services were mostly arranged in group with the average ratio of instructor: blind of 1:5 or 2:10. 45% of blind client aged >60 yrs, 55% was in range of 15-59 yrs. The functioning information after received O&M services was revealed. More than 90% of blind clients had no difficulty in performing daily activities and household ambulation. There still were some difficulties in doing instrumental or domestic activities e.g. cooking, gardening, shopping which age was statistical different factor. Most satisfying issues included improving ability to perform ADL and ambulation, increasing self-confidence, feeling good in health with more mobility in everyday life but least satisfied in increasing opportunity in education and vocational life areas. Collaborative organizations :