Download
1 / 21
220 likes | 1.09k Views
Definition. Hemolytic are a group of disorders characterised by shortened survival of RBCs in circulation .. An introduction. Consequences of hemolysisShortening of red cells survival does not always cause anemia as there is a compensatory increase in red cell production by the bone marrow.If the red cell loss can be contained within the marrow's capacity for increased output,then a hemolytic state can exist without anemia (compensated hemolytic disease). The bone marrow can increase its output25

E N D
1.
APPROACH TO A PATIENT WITH HEMOLYTIC ANEMIA
By
Dr. Ramlah Hasan
H.O MU-II
2. Definition Hemolytic are a group of disorders characterised by shortened survival of RBCs in circulation .
3. An introduction Consequences of hemolysis
Shortening of red cells survival does not always cause anemia as there is a compensatory increase in red cell production by the bone marrow.If the red cell loss can be contained within the marrow�s capacity for increased output,then a hemolytic state can exist without anemia (compensated hemolytic disease). The bone marrow can increase its output by 6 to 8 times by increasing the proportion of cells committed to erythropoiesis (erythroid hyperplasia) and by expanding the volume of active marrow. In addition, immature cells (reticulocytes) are released prematurly.
4. Sites of hemolysis
Extra vascular hemolysis
In most hemolytic conditions red cell destruction is extra vascular. The red Cells are removed from the circulation by macrophages in the reticuloendothelial system, particularly the spleen.
5. Sites of Hemolysis (contd.) Intra vascular Hemolysis
When red cells are rapidly destroyed within the circulation Hb is liberated. This is initially bound to plasma haptoglobin but these soon become saturated. Excess free plasma Hb is filtered by the glomerulus and enters the urine, although small amounts are reabsorbed by the renal tubules. In the renal tubular cells Hb is broken down and becomes deposited in the cells as haemosiderin.
6. Classification of Hemolytic Anemias Intra corpuscular
Hereditary
Membrane Defects
Hereditary Spherocytosis
Hereditary Elliptocytosis
Enzyme Deficiency
G6PD Deficiency
Pyruvate Kinase Deficiency
Haemoglobinopathies
Sickle Cells Anemia
Unstable Haemoglobins
Acquired
Paroxysmal Nocturnal Haemoglobinuria
7. Classification of Hemolytic Anemias Extra corpuscular
Autoimmune Hemolytic Anemias
Associated with warm antibodies
Associated with cold antibodies
Isoimmune Hemolytic Anemias
Drug induced Hemolytic Anemias
Infections
Plasmodiam, Clostridium
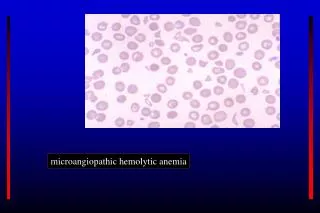
Microangiopathic Hemolytic Anemias
Hypersplenism
8. Clinical Approach History
Examination
Investigation
Treatment
9. History Age
Hemolytic anemia can occur at any age.
Hereditary disorders usually are evident early in life.
AIHA is more likely to occur in middle-aged and older individuals.
Sex
Most cases of hemolytic anemia are not specific to any gender.
Autoimmune hemolytic anemia (AIHA) is slightly more likely to occur in females than in males.
G-6-PD deficiency is an X-linked recessive disorder. Males usually are affected, and females are carriers
10. History (contd.) Symptoms
Pallor, Fatigue, Worsening of preexisting, angina, Palpitation, Postural dizziness
Mottled or Numb fingers or toes
Pigment gall stone
Reddish Brown first morning urine
Symptoms due to splenomegaly like dragging sensation in abdomen
Acute painful episode include the bones (especially the back and long bones) and the chest.
11. History (contd.) Family History
Positive Medical History for Associated Diseases
Drug Hsitory
Analgesics
Anti-malarials
Anti-bacterials
12. Examination Pallor
Jaundice
Tachycardia
Flow murmurs
Signs of congestive cardiac failure
Poorly healing ulcers over lower tibia
Splenomegaly
Cholelithiasis
13. Investigations Blood Complete Picture
Hb ? or N
TLC
PLT
Red Cell Indices
MCV
MCHC
Reticulocytosis
Bone Marrow Examination
Erythroid Hyperplasia
Serum Levels
Bilirubin
The level of unconjugated bilirubin never exceeds 4 to 5 mg/dl.
Haptoglobin
Plasma Haemoglobin
Lactate Dehydrogenase
Positive Urinary Haemosiderin
14. Peripheral Blood Film
15. Hereditary Spherocytosis
16. Sickle Cell Anemia
17. Other Investigations Osmotic fragility test
Specific enzymatic assays
Hb electrophoresis
18. Evaluation of Hemolysis
19. Treatment More than 200 types of hemolytic anemia exist, and each type requires specific treatment. Therefore, only the aspects of medical care relevant to most cases of hemolytic anemia are discussed.
Transfusion therapy
Avoid transfusions unless absolutely necessary, but they may be essential for patients with angina or severely compromised cardiopulmonary status.
Administer packed RBC slowly to avoid cardiac stress.
In AIHA, type matching and crossmatching may be difficult. Use the least incompatible blood if transfusions are indicated. The risk of acute hemolysis of transfused blood is high, but the degree is dependent on the rate of infusion. Slowly transfuse by administering half units of packed red cells to prevent rapid destruction of transfused blood.
Discontinuing medications
Discontinue penicillin and other agents that can cause immune hemolysis and oxidant medication such as sulfa drugs
20. Treatment (contd.) Administer folic acid because active hemolysis may consume folate and cause megaloblastosis.
Corticosteroids are indicated in AIHA.
IV immunoglobulin G (IgG) has been used for patients with AIHA, but only a few patients have responded, and the response has been transient.
Iron therapy
This is indicated for patients with severe intravascular hemolysis in which persistent hemoglobinuria has caused substantial iron loss.
Before iron is administered, document the iron deficiency by serum iron studies and, possibly, by assessing iron stores in bone marrow aspirates.
Because iron stores increase in hemolysis, iron administration generally is contraindicated in hemolytic disorders, particularly those that require chronic transfusion support.
21. Treatment (contd.) Surgical Care:
Splenectomy may be the first choice of treatment in some types of hemolytic anemia such as hereditary spherocytosis.
In other cases, it is recommended when other measures, such as in AIHA, have failed.
Splenectomy usually is not recommended in hemolytic disorders such as cold agglutinin hemolytic anemia.
Immunize against infections with encapsulated organisms, such as Haemophilus influenzae and Streptococcus pneumoniae, as far in advance of the procedure as possible.
22. Points to Remember Peripheral smear is the most important initial investigation and
Coombs test with anti-IgG and anti-complement in diagnosing hemolytic anemia.