Download
1 / 14
150 likes | 845 Views
Medical Staff CQI Memorial Hospital Chester, Illinois 3/26/09 Medical Staff Performance Improvement Process: Variety of Indicators which involve all Medical Staff: Active Staff ER Physicians Radiologist Consultants Source of indicators:

E N D
Medical Staff CQI Memorial Hospital Chester, Illinois 3/26/09
Medical Staff Performance Improvement Process: • Variety of Indicators which involve all Medical Staff: • Active Staff • ER Physicians • Radiologist • Consultants • Source of indicators: • Best practice Guidelines: (HQA, HOP QDRP, etc. ) • COP/JC Standards (V.O., Timely H &P, H & P Update) • National Patient Safety Goal Compliance • Physician approved protocols • Data collected by various disciplines throughout the hospital; for example: • Blood Utilization (Lab) • Clinical indicators (OR, ER) • Core Measures: PI director • Incident Reports: Safety Director • Medical Record Review: HIM director • Utilization Review: UR Mgr.
Process continued: • The overall results of the indicators are then reported to: • PI committee, • Environment of Care Committee. • From these two committees, the overall results are then forwarded to the Medical Staff Committee of the Whole.
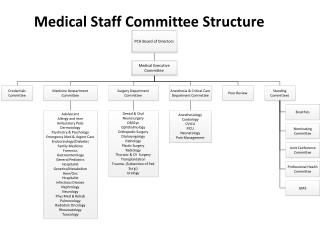
Peer Review Process: • Any indicators that result in variation are referred initially to the Physician Advisor, • Examples: • Blood Utilization: Lab Advisor • IP Core Measures: Chief of Staff • Trauma Indicators (ER): ER Physician Director • Vancomycin: Infection Control Advisor. • Physician Advisor determines if further review is warranted by the Peer Review Committee. • If further review warranted: • Sent on to Quarterly Peer Review Committee Meeting. • Peer Review committee takes further action as warranted: • Continuing education, monitoring, focused practice evaluation. • Form to track record as it moves through this process
MEMORIAL HOSPITAL CHESTER, ILLINOIS PHYSICIAN REVIEW FORM Patient Name: DOB: M#: Date of Admission/Occurrence: Physician Involved: Committee Recommending the Review: ******************************************************************************************************* PHYSICIAN REVIEW Date reviewed: Physician Reviewer: Recommend for Peer Review Committee? _________________Yes _________________No Comments: ******************************************************************************************************* PEER REVIEW COMMITTEE Date Reviewed by Committee: Comments/Recommendations: Chief of Staff:__________________________________________________________________________________________ Signature Date ***************************************************************************************************** FOLLOW UP Supporting documentation of follow up actions, activity, monitoring, education, or other relevent information may be attached as indicated. Chief of Staff:_______________________________________________________________________________________ Signature Date PRIVILEGED & CONFIDENTIAL: All information provided on this form, including any appended materials, is Privileged & Confidential, to be used solely in the course of internal control and for the purposes of reducing morbidity and mortality and improving the quality of patient care, as provided in the Illinois Medical Studies Act 735 ILCS 5/8-2101.
Indicators: • Core Measures: • IP: • AMI, CHF, Pneumonia, SCIP • OP • Chest Pain, AMI, Out Patient Surgery. • Tissue Review: • Normal tissue, too little tissue, clear margins, etc. • Blood utilization: • Hgb below 8.2; Platelets, FFP, etc • Documentation of informed consent, written orders • Incident Reports • Physician complaints. • Sentinel Event.
Indicators: continued • Medication Usage: • Significant clinical interventions • Anticoagulation Protocol • Vancomycin Usage • Infection Control • HAI • Vancomycin Usage • Medical Record Review • Dating, timing, signing Verbal and Telephone orders • Prohibited abbreviations • Delinquent Records • H & P’s; Update to H & P • Complete/Timely Operative Report/Operative note • Timely consultant dictation
Indicators: • ER Physician Indicators: • Trauma Indicators • Chest pain / AMI • Timeliness of Thrombolytics, • X-ray interpretation • ER Management / Documentation issues • Utilization Management • LOS • Readmissions • Admission/Continued stay criteria not met. • Denials • RAC Audits ?? • Mortality/Morbidity Review
Indicators: Continued • Surgical and other invasive procedures: • Timely H & P; update • Universal Protocol • Informed consent • Pre-op / Post-op discrepancies including path diagnosis • Conscious Sedation Outcomes • Deaths in OR/PACU • Repairs, lacerations, Perforations, Tears • Anesthesia indicators • Retained foreign body • Returns to OR in 24 hours.
Hospital Quality Alliance Memorial Hospital Ref: Joint Commission’s Medical Staff Standards. Sponsored by Illinois Hospital Association.
Hospital Quality Alliance Memorial Hospital Ref: Joint Commission’s Medical Staff Standards. Sponsored by Illinois Hospital Association.
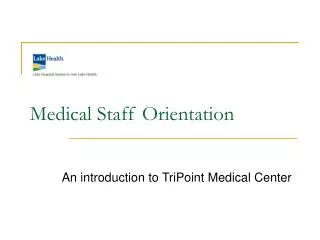
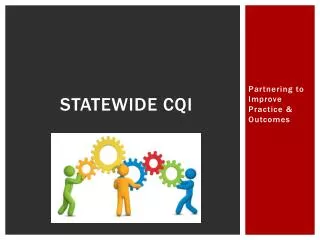
Credentialing: • Summary of all indicators is compiled for each physician. • Summary attached to Medical Staff Re-application. • Reviewed by Medical Staff when physician is recredentialed. • See Summary Form
PHYSICIAN SUMMARY MEMORIAL HOSPITAL, CHESTER, IL PHYSICIAN: ____________________________________ Year:_________________________ YEAR TO DATE: PATIENT CARE ACTIVITIES: # Admissions # Discharges # Observation Patients # Procedures: # Deaths: # Del Charts: ALOS HOSPITAL QUALITY ALLIANCE: Congestive Heart Failure:......................................................................................................................................100% Discharge Instructions:........................................................................................................................................90% LVF Assessment: ...............................................................................................................................................100% Smoking Cessation:.............................................................................................................................................100% Pneumonia: Antibiotics within 4 hours of arrival:...................................................................................................................90% Appropriate Selection of Antibiotics: ................................................................................................................100% Blood Culture prior to Antibiotics: ....................................................................................................................100% Influenza Vaccine: -----------------------------------------------------------------------------------------------------------80% Pneumonia Vaccine: --------------------------------------------------------------------------------------------------------100% Oxygenation Assessment: Adult Smoking: Prot Ordered: Acute Myocardial Infarction: Aspirin on Arrival: Aspirin at Discharge: Beta Blocker on Arrival: Beta Blocker at Discharge PATHOLOGY REVIEW: Tissue Adequate:.....................................................................................................................................................96% Biopsy Justified....................................................................................................................................................... 4%
MEDICATION REVIEW: # of Medication Interventions......................................................................................................................................0 Appropriate Use of Vancomycin:...........................................................................................................................100% BLOOD/BLOOD COMPONENT REVIEW: Approved Indicator Met for Transfusion:.............................................................................................................. Reviewed by Pathologist and Approved: ............................................................................................................. Written Order for Blood Transfusion:................................................................................................................... Documentation of Informed Consent:................................................................................................................... CLINICAL PERTINENCE: Timely H & P:..................................................................................................................................................... Operative Report Dictated Day of Surgery: ........................................................................................................ Operative Note Written Immediately post op: ................................................................................................... Timely Clinical Resumes ................................................................................................................................... Timely Surgical H&P:........................................................................................................................................ PHYSICIAN ADVISOR REVIEW Reason for review: Outcome - Refer to Peer Review Committee? PEER REVIEW COMMITTEE: Reason for Review MEETINGS - % ATTENDED: Medical Staff Meeting Committee of the Whole: .................................................................................................... Medical Conference: Peer Review: ........................................................................................................................ Special Committees: Mortality & Morbidity: