Download
1 / 16
180 likes | 377 Views
Preimplantation analysis of kidney biopsies from expanded criteria donors. Amaia Sagasta, Ana Sánchez-Escuredo, Frederic Oppenheimer, Manel Solé Department of Pathology and Kidney Transplant Unit, Hospital Clínic, Barcelona, Spain.

E N D
Preimplantation analysis of kidney biopsies from expanded criteria donors Amaia Sagasta, Ana Sánchez-Escuredo, Frederic Oppenheimer, Manel Solé Department of Pathology and Kidney Transplant Unit, Hospital Clínic, Barcelona, Spain * DISCLOSURE OF INTEREST: The authors report no conflicts of interest.
Introduction I • Patients with end-stage renal disease attain longer life expectancy and better quality of life through kidney transplantation • Critical shortage of kidneys for transplantation > 60 y 45-60 y 30-45 y 15-30 y < 15 y ONT 2011
Introduction IIECD group definition Efforts to expand the kidney donor pool Incorporation of expanded criteria donors (ECD) • Age ≥ 60 years • OR • Age 50-59 years with ≥ 2 risk factors : • Death by cerebrovascular accident • History of hypertension • Creatinine level > 1.5 mg/dL
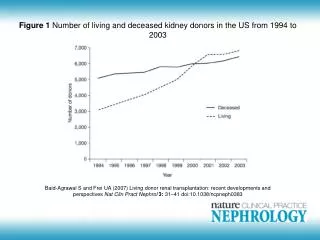
Introduction IIIECD group associated problems Suboptimal post-transplant function Shorter graft survival Careful selection of the grafts before trasplantation Preimplantation kidney biopsy in ECD *Sung RS, et al. Transplantation. 2005 May 15;79(9):1257-61 #ONT 2011
Introduction IVIB practice and interpretation • Scores in use: • Remuzzi score (Rs): • Glomerular global esclerosis (GS), tubular atrophy (TA), interstitial fibrosis (IF), arterial and arteriolar narrowing (CV) • Banff score based modifications: • Arteriolar hyalinosis (AH), mononuclear cell interstitial inflammation (ii) • Techniques in use: • Frozen sections, Paraffin sections Interobserver variability Lack of universally accepted practice guidelines for biopsy processing and interpretation of the histological findings
Aim of the study • To analyze the correlationbetween: • Different observers, using frozen sections • Different techniques: paraffin vs. frozen (same observer) • To analyze if the modification of the score parameters could improve the correlation: • Analysis of an alternative score (As) • Alternative GS parameter • Combined tubulo-interstitial parameter • AH parameter
Original report • Pathologist-on-call: Several general pathologists • Time of transplantation • Frozen section
Materials and Methods II Scoring of biopsies GS: RsAs 0= none 0= none 1= <20% 1= 1-10% 2= 20-50% 2= 11-20% 3= > 50% 3= > 21% IF: 0= ≤ 5% 1= 6-25% 2= 26-50% 3= > 50%. TA: 0= absent 1= ≤ 25% 2= 26-50% 3= > 50%. AH: 0= absent 1= mild to moderate in at least one 2= moderate to severe in >1 3= severe in many CV: 0= absent 1= ≤ 25% 2= 26-50% 3= > 50%.
Materials and Methods IIIElegibility; statistics • Elegibility for transplant or discard (biopsy): • ≤ 4 points Remuzzi score: acceptance / >4 : discard • Statistics for concordance in organ elegibility analysis: • Kappa index (K): values between 0 (no agreement) and 1 (perfect agreement) • Statistics for correlationanalysis (parameters, scores): • Kendall’s Tau b (KTb): values between -1 (perfect disagreement) and 1 (perfect agreement), 0 (absence of association)
Results I - Parameters PS: parraffin sections (PAS); FS: frozen sections (H/E)
Results II - Scores PS: parraffin sections (PAS); FS: frozen sections (H/E)
Results IIIConcordance in organ acceptance PS: parraffin sections (PAS); FS: frozen sections (H/E); ORFS: original report frozen section (H/E) • Importance of observed differences in organ acceptance: • FS revisiona posteriori by single observer would have resulted in 9.75% more discard than ORFS • FS revision would have resulted in 7.6% more discard than PS revision by the same observer
Conclusions • The evaluation of the score items by a single, trained observerimproved the correlation in all values, despite the use of different techniques • Remuzzi score was the parameter with the best improvement in correlation • Given the relevance of the observed differences in organ acceptance, specific training is advisable irrespective of the technique used
Thank you for your attention asagasta@clinic.ub.es
References • Remuzzi G, Grinyo J, Ruggenenti P et al. Early experience with dual kidney transplantation in adults using expanded donor criteria. Double Kidney Transplant Group (DKG). J. Am. Soc.Nephrol. 1999; 10; 2591–2598. • Perico N, Ruggenenti P, Scalamogna M, Remuzzi G.Tackling the shortage of donor kidneys: how to use the best that we have. Am.J.Nephrol.2003;23:245-259. • Munivenkatappa RB, Schweitzer EJ, Papadimitriou JC et al. The Maryland aggregate pathology index: a deceased donor kidney biopsy scoring system for predicting graft failure. Am. J.Transplant. 2008; 8; 2316–2324. • El-Husseini A, Sabry A, Zahran A et al.Can Donor implantation renal biopsy predict long-term renal allograft outcome?Am.J.Nephrol.2007;27:144-151 • Snoeijs MG, Boonstra LA, Buurman WA et al.Histological assessment of pre-transplant kidney biopsies is reproducible and representative. Histopathology 2010;56;198-202. • Sung RS, Christensen LL, Leichtman AB et al.Determinatns of discard of expanded criteria donor kidneys: impact of biopsy and machine perfusion. Am.J.Transplant.2008;8:738-792. • Furness PN, Taub N, Assmann KJ et al. International variation in histologic grading is large, and persistent feedback does not improve reproducibility. Am. J. Surg. Pathol. 2003; 27; 805–810. • Organización Nacional de Transplantes (ONT) Database