Download
1 / 46
460 likes | 663 Views
Chapter 14: The Pharmaceutical Industry Health Economics. Outline. Competitiveness of the pharmaceutical industry Conduct Performance. Benefits of Drugs. Reduce mortality. Reduce morbidity/improve quality of life. Reduce cost of treating diseases. Industry Structure.

E N D
Outline • Competitiveness of the pharmaceutical industry • Conduct • Performance
Benefits of Drugs • Reduce mortality. • Reduce morbidity/improve quality of life. • Reduce cost of treating diseases.
Industry Structure • # and size distribution of sellers. • Buyers’ side characteristics. • Barriers to entry. • Government regulation.
Leading Pharmaceutical Companies, 2000 Company Sales $b Merck 40.3 Johnson & Johnson 29.1 Pfizer 29.6 Bristol-Myers Squibb 21.3 Pharmacia 18.1 Abbott Laboratories 13.7 American Home Products 13.8 Eli Lilly 10.9 Schering-Plough 9.8 Amgen 3.6 Fortune Magazine, 2001
Can competition be accurate measured at the industry level? • Most drugs are not substitutes to the patient. • The relevant product market is the therapeutic market. • Only a few major drugs compete in most therapeutic markets. • Concentration ratios at this level are higher than for industry as a whole.
Firms tend to make most profits from 1 or a few key drugs. BCG, The Changing Environment for U.S. Pharmaceuticals, 1993
How 3rd parties influence drug demand • Even if consumers exert little influence over drug choice, 3rd parties are making the market more competitive. • Formularies - list of selected drugs physicians may prescribe. • Used by hospitals to limit inventories and costs. • Used by most HMOs and many PPOs. • Used by many state Medicaid programs.
Drug utilization review • Used by insurers to enforce formularies, identify inappropriate prescribing practices. • Government influence • 1990 Omnibus Budget Reconciliation Act - Federal funding provided for drug only if state Medicaid program receives manufacturer rebate agreement
Government influence (cont.) • 1992 Veterans Health Care Act - price discounts for Federal Supply Schedule, VA, Dept. of Defense. • These programs may restrict costs for government, but drug firms may be forced to raise nonfederal prices.
“…managed care emphasizes less-expensive, preventive types of treatment.” “The rate of growth for drugs to treat high blood pressure and high cholesterol in certain managed-care strongholds on the West Cost has gone off the charts.” WSJ 10/17/96
“Consumers in the $94 billion prescription drug market are mostly indifferent to price. What will happen when they all become budget conscious? Forbes 4/5/99
Pharmacy Benefit ManagersGeneral Strengths • Information - e.g. Medco’s 60m patients. • How drugs prescribed, used, impact on disease. • Can prevent inappropriate drug interactions, under/over medication • PBMs provide drugs at lower costs. • Achieve econ. of scale in pharmacy benefits by serving multiple plan sponsors. • Large market share on buyer’s side stronger negotiating power w/ drug companies.
Vertical Integration • Brand name drug companies are purchasing PBMs.
Vertical Integration • Good or bad idea? • Buy the information, not the PBM • “Industry consultants and Medco competitors argue that Merck could have bought that information from Medco or others in the field without buying the company.” NYT 8/5/93 • Critics argue that PBMs will only serve to lower prescription pharmaceutical prices.
Vertical Integration • Comments from Roy Vagelos, former Merck CEO • “In classic terms of competition, we could see that the power of the buyers was growing…PBMs were…bringing together the person who chooses the drug and the person who pays for the drug.” • “Having salespeople visit doctors’ offices does not allow us to reach PBMs, HMOs, or plan sponsors -- the major players in the emerging market.”
Vertical Integration • Merck bought Medco as a response to managed care. • Strategic attempt to market power. How? • Followup on patients w/ chronic illness who may stop taking prescribed meds. • Position Merck drugs favorably on formulary. • e.g. lower patient copay, or lower cost to plan sponsor.
Vertical Integration • Offer risk sharing to demand. • e.g. refund Proscar if no effect on BPH after 1 year. • Offer disease management. • Improves patient health, gives company more influence in tx process.
Vertical Integration • PBM purchase will also affect Merck’s product development. • “Consider what happens if instead of having 20 products on the formulary we have 40.” • more incentive to develop generics. • Impact of PBMs on drug prices: • Price competition is inevitable. • “Merck will have to grow through increased volumes without considerable price increases. That seems obvious now, but it wasn’t six or seven years ago.”
Barriers to entry • Government patents. • Brand loyalty advantage. • Control over a key input.
Government Patents • Innovating firm gains the right to be sole producer of a drug for legal maximum of 20 years. • Preserves incentives for firms to undertake risky and costly research and development (R&D) that is socially valuable. • Rationale: Monopoly restriction of output better than having no output at all.
Monopoly power of patents is not always strong. • Patents granted for chemical composition, not therapeutic novelty. • Tagamet & Zantac both were patented, competing in antiulcer market. • Significant part of patent life may be spent trying to get FDA approval. • “effective” patent life = 8 years.
Monopoly power of patents is not always strong. • 1984 Waxman-Hatch Act - benefits for both brand-name and generic companies. • Effective life of new drug patent can be extended up to 5 years of FDA delayed market introduction. • Fast approval process for generics: eliminated proof of safety & effectiveness.
Pharmaceutical Industry Conduct • Pricing • Does more intense competition drug prices? • Promotion • Does drug advertising promote or impede competition? • Product innovation • Are large firms necessary for drug innovation? • Preview: Empirical evidence indicates that competition is at work, but the industry does not exhibit perfect competition.
Pricing Behavior • Can the brand-name firm maintain its price once its patent expires and generics enter? • Average price differential between brand-name and generic firms = 127%, but brand name market share = 63.4%.(Hurwitz & Caves, 1988) • Branded drugs’ prices 11% 2 years after generic entry. (Grabowski & Vernon 1992) • Yet brand-name drugs lost 1/2 of market share. • Average market price fell to 79% of pre-entry price.
Pricing Behavior • Brand-name firms segment the market. • Remaining customers relatively price insensitive. • Inelastic demand curve allows them to maintain price.
Promotion Strategies • Promotion Magnitude: • Research-base firms spend as much as 20-30% of sales on promotion. • 70% pharmaceutical salespersons (detailing). • 27% advertising. • 3% direct mail. • Impact: • 22,000 drugs on market timely, valuable information. • May impede competition.
Product Innovation Www.phrma.org
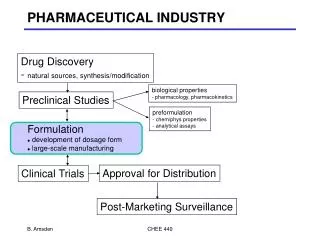
Product Innovation • Innovation is very risky and time consuming. • R&D process takes many years. • Only a small fraction of new drug discoveries are eventually marketed. • 75% of NCEs in Phase 1 go to Phase 2. • 36% of NCEs in Phase 1 go to Phase 3.
Roy Vagelos’ Views on R&D • Priority areas are those where: • No therapies or drugs are available. • Science must be advanced enough to make a breakthrough. • Must have enough knowledge of the disease to have an idea how to arrest it. • Rational drug discovery - create specific molecules to attack specific molecular drugs. • Enzyme inhibition, which was successful in Merck drugs treating high cholesterol, high blood pressure, and prostate disease.
Pharmaceutical Industry Performance Does the absence of perfect competition higher prices & restricted output?
Cautionary note on inflation • The inflation rate calculated by BLS is based on a price index, which may overstate the true in drug costs. • Price index • the relative cost of purchasing a fixed “basket” of drugs in year t, vs. the costs of same basket in a base period. Price Indext =
Cautionary note on inflation • BLS “basket” undersamples new drug products, which generally have smaller price increases than older drugs. • BLS treats generics as new products, not as substitutes for more expensive drugs. • BLS uses list rather than transactions prices. • BLS doesn’t adjust prices to reflect quality improvements.
Are profits in the drug industry too high? • Under standard accounting practices, R&D is written off as a current expense. • But R&D affects revenues for years to come. • Rate of return on investment is calculated using an asset base that improperly excludes intangible R&D. • Should capitalize R&D outlays & depreciate them over appropriate time periods. • Accounting figures overstate the rate of return on assets for drug companies.