Download
1 / 33
330 likes | 362 Views
Learn about Scapular Muscle Detachment, its rarity, diagnosis, treatment, and outcomes post-surgery. Detailed insights from Dr. Ben Kibler's research and clinical studies. Recognize symptoms, surgical techniques, and long-term effects.

E N D
SCAPULAR MUSCLE DETACHMENT Say what? Is this real? How do I treat it
W. Ben Kibler, MD Medical director
W. Ben Kibler, MD • Shoulder Center of KY • Disclosure • Disorders of the Scapula and Their Role in Shoulder Injury
Scapular Muscle Detachment Previously rarely recognized CORR 1987 My first case 1997- post op snapping ? Incidence, prevalence Poorly diagnosed, treated Lack- recognition, effective treatment Multiple sequelae, poor function
Clinical clues Post traumatic localized highly painful area- medial border, +/- defect Snapping, G-H derangement (results) Altered function- relief by SAT, SRT Chronic pain response
21 y.o. 3 years post MVA, pain 6-8/10 localized to medial border, weakness, inability to raise arm > 90, multiple PT, injections, MRI negative
Pathology- rhomboids, low trap Tenuous tissue attachment Scar, hypervascular attachment Treatment- re-attachment through pairs of drill holes Medial border Scapular spine
Detachment Lower Trapezius Muscle Medial Scapular Border Scapular Spine Infraspinatus Muscle Head Foot
Retractor/Protector Detachment Infraspinatus mobilized off medial border of scapula
First pass of 2nd mattress suture Mattress Suture
Detachment attached to medial border Lower trapezius attached to spine Infraspinatus re-attached
Clinical outcomes Kibler et al JSES 2014 Kibler et al JSES 2108
Prospective, N= 78 ASES- pain, function scales Intake, during, discharge, 2- 3 year follow up Presentation, exam, surgical findings Kibler et al JSES 2014
JSES 2014 Injury mechanism Number (%) MVA 35 (45) Traction/load 19 (24) Athletics 15 (19) Other 9 (12)
JSES 2014 Patient reported complaints Localized medial border scapular pain- 78 (100%) Decreased overhead activity capability- 77 (99) Decreased forward flexion capability- 76 (97)
JSES 2014 Patient reported complaints Headaches/muscle spasms- 67 (86) Inability- work activities- 60 (75) Decreased flexion strength- 52 (67) Decreased abduction/over head strength- 46 (59)
JSES 2014 Sx duration 51(1.5- 372) months 4 (1- 20) other physicians 1 (0-6) other surgeries PT 14 (1- 42) months 3 (2 CT, 1 MRI) imaging positive for muscular injury
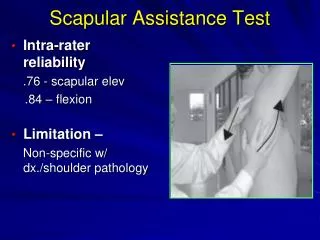
JSES 2014 Physical exam findings Dyskinesis- 78 (100) Medial border pain- 76 (97) (+) SRT- 76 (97) (+) SAT- 76 (97)
JSES 2014 Physical exam findings Can’t raise > 90- 75 (96) Weak rotator cuff- 59 (76) Palpable defect- 47 (60) (+) impingement- 40 (51)
JSES 2014 2- 3 year ASES scores (N=34) Intake/Discharge/Follow up Pain 20/34/35 P<.0001 Function 19/30/34 P<.0001 Total 39/63/69 P<.0001
JSES 2018 • Longer follow up- subgroups • ASES pain, function, total • GROC, satisfaction (0- 10) • Pain- PCS- catastrophization • Non catastrophizers- PNC • Catastrophizers- PC
JSES 2018 3- 5 year ASES scores (N=48) Intake/Follow up Pain 21/38 P<.0001 Function 19/35 P<.0001 Total 39/73 P<.0001
JSES 2018 PNC- 33 PC- 15 Intake/Follow up Pain 20/43* 23/27 Function 22/39* 20/24 Total 42/83* 43/52
JSES 2018 GROC+ 2- moderate change Satisfaction NS- 0- 3/10, MS- 4- 6/10, HS- 7-10/10 NS= 9 (7- PC), ASES 41/44 MS= 10 (5- PC), ASES 41/66* HS= 29 (3 PC), ASES 43/85*,**
Conclusions Specific clinical syndrome Major activity/life disruption Consistent history, physical exam, symptoms, clinical dysfunction Imaging not helpful Consistent surgical findings
Conclusions Significant improvement, pain, function, surgical technique important Short term, long term Psychological effects may have major determinant role Evaluate, treat- co-morbidity
Conclusions More awareness- clinical presentation Recognize the acute injury and start definitive treatment early in injury course so that the long term problems don’t get established
THANK YOU www.shouldercenterofky.com