Download
1 / 21
220 likes | 387 Views
Interpretation of CT Brain- neuro surgical prospective. Dr A Gazdar 04/09/2013. CT. Sliced angled images of brain from skull base to vertex. Either cross sectional (axial) / coronal / sagittal images Radiocontrast used is iodinated : !!!allergy. Normal anatomy. A. Frontal Lobe

E N D
Interpretation of CT Brain- neurosurgical prospective Dr A Gazdar 04/09/2013
CT Sliced angled images of brain from skull base to vertex. Either cross sectional (axial) / coronal / sagittal images Radiocontrast used is iodinated : !!!allergy
Normal anatomy A. Frontal Lobe B. Frontal Bone (Superior Surface of Orbital Part) C. Dorsum Sellae D. Basilar Artery E. Temporal Lobe F. Mastoid Air Cells G. Cerebellar Hemisphere
A. Frontal Lobe B. Sylvian Fissure C. Temporal Lobe D. Suprasellar Cistern E. Midbrain F. Fourth Ventricle G. Cerebellar Hemisphere
A. Falx Cerebri B. Frontal Lobe C. Anterior Horn of Lateral Ventricle D. Third Ventricle E. Quadrigeminal Plate Cistern F. Cerebellum
A. Anterior Horn of the Lateral Ventricle B. Caudate Nucleus C. Anterior Limb of the Internal Capsule D. Putamen and Globus Pallidus E. Posterior Limb of the Internal Capsule F. Third Ventricle G. Quadrigeminal Plate Cistern H. Cerebellar Vermis I. Occipital Lobe
A. Genu of the Corpus Callosum B. Anterior Horn of the Lateral Ventricle C. Internal Capsule D. Thalamus E. Pineal Gland F. Choroid Plexus G. Straight Sinus
A. Falx Cerebri B. Frontal Lobe C. Body of the Lateral Ventricle D. Splenium of the Corpus Callosum E. Parietal Lobe F. Occipital Lobe G. Superior Sagittal Sinus
A. Falx Cerebri B. Sulcus C. Gyrus D. Superior Sagittal Sinus
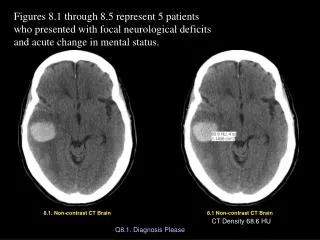
Trauma Both brain and bone windows need to be examined Fractures are noted in sinuses, skull base, mastoid bone, temporal (petrous), skull. Either linear or depressed. Either displaced or undisplaced
SAH Most commonly associated with vascular anomalies Aneurysm, AVM CT grading is Fischer grade
Acute SDH NSx emergency Crescent shaped Hyperdense, may contain hypodense foci due to serum, CSF or active bleeding Does not cross dural reflections
EDH Associated with skull fractures Hyerdense biconvex Can cross the dural borders
contusions ill-defined hypodense area mixed with foci of hemorrhage. Adjacent subarachnoid hemorrhage is common. >24-48 hours, hemorrhagic transformation or coalescence of petechial hemorrhages : evolution
tumors Contrast needed to delineate Multiple at grey white junction– mets Dural based – meningioma Diffuse intraparenchymal – high grade gliomas
hydrocephalous Communicating or obstructive Trapped horns Look for cause Associated hardware
Intracranial infections Abscess – extra or intra cranial Extra : look for sinusitis, thrombophlebitis, postop Intra: look for distant source
Nerve wreck….. Describe the lesion…
Thank you.. Have a great day!!