Download
1 / 47
480 likes | 864 Views
Ch. 5- DMI 56 Gastrointestinal System. Marilyn Rose RT, RDMS. Outline. Physiology of Digestive System Esophagus Stomach Small Bowel Colon Gallbladder Liver Pancreas Pneumoperitoneum spleen. Physiology.

E N D
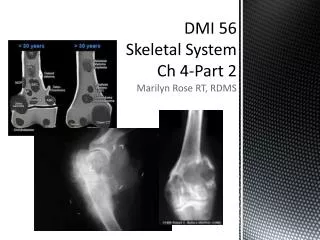
Ch. 5- DMI 56Gastrointestinal System Marilyn Rose RT, RDMS
Outline • Physiology of Digestive System • Esophagus • Stomach • Small Bowel • Colon • Gallbladder • Liver • Pancreas • Pneumoperitoneum • spleen
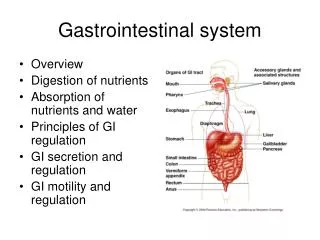
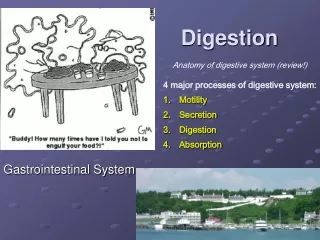
Physiology • Basic function- alter chemical/ physical composition of food so it can be absorbed and used by body cells • Digestion • begins with mastication in the mouth • Salivary secretions moisten food • Deglutition or swallowing is a coordination of many muscles and sphincters • Stomach churns contents into chyme with hydrochloric acid and pepsin • Peristalsis propels contents into the duodenum • Greatest digestion occurs in the duodenum • Intestinal secretions of mucus and enzymes
Physiology contd. • Pancreas secretes the enzymes • trypsin and chymotrypsin for proteins • Lipase for fat • Amylase for carb • Alkaline solution to neutralize the acid carried into small bowel from sto • Liver- secrete bile and store in the GB • GB – CBD enters duodenum • Bile emulsifier – dispersing fat into droplets to mix with water • Digestion complete when absorbed by intestinal mucosa (villi= >surface area) and into blood capillaries and lymph vessels of wall of small bowel • Not digested material passes into colon where water and minerals are absorbed and remaining matter is excreted
Physiology of Liver, GB, Pancreas • Liver • Largest gland- detoxify poison- ammonia, alcohol, barbiturates • Secrete 1 pint of bile per day • Essential for absorption of fat and vitamins- A, D, E and K • Metabolism of protein, fats and carbohydrates • Synthesis of enzymes- albumin, & blood clotting- fibrinogen, prothrombin • Liver damage results edema • Maintain glucose- take excess glucose (smint) and store as glycogen • Glucose drops in blood- reverse happens and glycogen is broken down to glucose • Store iron, vitamins A, B12 and D • GB • Function to store bile from hepatic and cystic ducts- concentrate bile by absorbing water • Contracts and ejects bile into duodenum in the presence of fat • Pancreas • Secrete insulin a glucagon- islets of langerhans • > glucose= > insulin • Pancreatic duct excretes enzymes to break down protein, carb and fat
Pathology of the esophagus • TEF • Esophagitis • Esophageal Cancer • Esophageal diverticula / varices • Hiatal hernia • Achlasia • Foreign body • Perforated esophagus
TEF • Congenital • Failure of lumen to develop separate from trachea • Blind pouch- cong espohatresia • Involved with skeletal, cardio and GI anomalies • Type 1- • up/ low blind pouch- no air below diaphragm • Type 2- • up- communicate with trachea- lower blind pouch • No air within the abdomen on KUB • Type 3- most common • up- blind pouch/ low attached to trachea by fistula • air enters through fistula • air seen below the stomach on KUB • Type 4- two types • First • up/low end in blind pouches • both connected to trach/bronch tree • Gas is seen in the stomach • Second- H fistula • both trachea and esophagus are intact • The two are attached by a fistula-level of cricoid • Can be missed until adulthood • CT is the best method to evaluate and less invasive than contrast studies • Acquired- malignancy, infection or trauma • 80% die within 3 months
esophagitis • Reflux (GERD) • Alcohol, chocolate, caffeine and fatty foods • relax sphincter • Acute- simulate heart disease by burning chest pain • Superficial ulcers, dilated esoph, loss of effective peristalsis • Higher chances with sliding hiatal hernia • Radiographic: • Demonstrate on esophagram- valsalva (may not see) • Hiatal sac • Hazzy border- erosions • Barrett’s Esophagus • Squamous lining of lower esoph destroyed- columnar • High malignancy risk in columnar lining (adeno-5%) • Radiographic • Variable length of normal esoph- ulcer or stricture in up esoph • Candida/ Herpes • Occurs in CA, radtx, chemo, immunocomp/ AIDS • Radiographic • Cobblestone, deep ulcerations, shaggy • Corrosive agent ingestion • Alkaline/acidic • Superficial- minimal ulceration, strong alkaline- deep lesions
Esophageal cancer • Progressive difficulty in swallowing (dysphagia) - >40 >men • Symptoms appear late in the disease • Direct extension of tumor usually has occurred by time of dx • Squamous cell- dismal prognosis • Esophogastric junction • Excessive alcohol and smoking • Radiographic • Flat plaque-like lesion- one wall of esophagus • Early form can be missed • Advanced lesions encircle lumen • Less common is polypoid lesion • Proximal dilation of esop- asipration pneumonia • Fistula formations- esoph and trachea • >3-5 mm wall thickening on CT is abnormal • CT stage- size, extension, resectability • Tumor spread- obliterate fat plane-esoph and lt atrium, AO • Fistula- tracheobronchial tree • Low density masses in liver, >lymph nodes • Radiographic contrast
Esophageal diverticula/ varicies • Diverticula • Outpouching (s) – common lesions • Composed of all layers or just mucosa/ submucosa • Small diverticula do not retain food/ secretions- asymptomatic • When diverticulum gets large and fills with food- aspiration pneumonia • Radiographic • Zenker’sdiverticulum- arise from posterior wall of upper cervical esoph • Occasionally very large and can occlude lumen • CT best demonstrates involvement of structures • Epiphrenicdivereticulm are found in the distal 10 cm of esoph- peristalsis • Varicies • Dilated veins in walls of the esophagus • From increased pressure in portal venous system (PHTN) • Result of cirrhosis of liver • Collateral formation of esoph and gastric varicies • Radiographic • Serpiginous- wavy border of walls • Thickening of folds- round fillings • Rosary beads • Barium overfilling may hide varicies • Upright or recumbent is best position • Endoscopic US • Main complictaion is bleeding
Hiatal Hernia • Most common abnormality- 50% of pop • Upper GI • Stomach in thoracic cavity • Predisposition to volvulus • Related to intraabdominal or intrathoracic pressure • Sliding Hiatal hernia • Complications • Esophagitis, ulcer, stenosis- mainly from reflux, not hernia • Radiographic • May appear on chest xray- soft tissue mass of posterior mediastinum • Prominent air/ fluid level • Mucosal folds- linear and parallel • Sometimes a ring encircles the distal esoph- Schatzki’s Ring- can be dilated
Achlasia • Functional obstruction of distal esophagus • Proximal dilation • Incomplete relaxation of esophageal sphincter • Related to absence of ganglion cells in distal esoph wall • Radiographic • CXR- dilated, tortuous esophagus • Widened mediastinum- air fluid level on Rt side, adjacent to cardiac shadow • Barium study- gradually tapered, smooth, conical, 1-3 cm narrowing of distal esoph- “rat tail or beak”
Foreign Body • Wide spectrum • Cervical – thoracic inlet • Unable to swallow without regurgitation • Metallic objects- coins, pin, small toys- radiopaque • Aluminum- may not see on xray • Suspected foreign body- • 2 projections - make sure it is inside the lumen • Radiographic • Food bolus- ingest barium • Above diaphragm- distal stricture • Intraluminal filling defect- irregular • May resemble a carcinoma
Perforation of the esophagus • Complication of esophagitis, peptic ulcer, neoplasm, external trauma or instrumentation • Most common cause- severe vomiting • Complete rupture can mimic myocardial infarction
Pathology of the stomach • Gastritis • Pyloric Stenosis • Peptic ulcer • Cancer of the stomach
Gastritis • Inflammation of the stomach • Irritants- like alcohol, corrosive agent, infection • H pylori- chronic gastritis- lead to peptic ulcer formation • Radiographic • Achohol- thick gastric folds, erosions • Corrosive- fibrosis and scarring- narrow antrum- gastric outlet obstruction • Bacterial- thickening of wall- narrow stomach • Infectious- gas bubbles from bacteria in stomach wall • Chronic atrophic- mucosal atrophy- absence of folds- pernicious anemia, malnutrition, medication, age
Pyloric stenosis • Infantile hypertrophic pyloric stenosis (IHPS) • Gastric antrum and pyloric canal become lengthened • Causing complete obstruction • Pyloromyotomy is done to open it
Peptic ulcer • Group of inflammatory processes of stom and duodenum • Caused by acid and pepsin • Occurs in lesser curvature • Complications • 20% hemorrhage (most common acute Up Gi bleed) • 5-10% gastric outlet obstruction (most common narrow lumen) • < 5% perforation (most common for pneumoperitonuem) • Types • Dudenal ulcer • Gastric ulcer • Superficial gastric erosions
Peptic ulcer types • Duodenal • Most common peptic ulcer dz- • >95% occur in first portion of duo bulb- beign • Radiographic • Demonstrate ulcer crater • Round or linear collection of contrast surrounded by lucent folds that radiate towards the crater • Secondary - thickening of mucosal folds and deformity of duo bulb • Acute cause muscular spasm – inconsistent margins of bulb • Chronic causes a fixed deformity of fibrous scarring/ narrowing at bullb- “cloverleaf” • Gastric • Occur in lesser curvature of stom- 5% malignant • Radiographic • Benign- projection of ulcer outside of the normal barium-filled gastric lumen- thin lucency • With radiating folds to the edge of the crater- smooth and slender- heal completely • Malignant- demonstrate irregular folds that merge into a mound of polypoid tissue • All ulcers in gastric fundus above esophagogastricjxn are malignant- never fully heal • Superficial gastric erosions • So small and shallow they are rarely demonstrated on conventional UGI • Cause: alcohol, antiinflammatory drugs, Crohn’sdz and candidiasis
Stomach Cancer • Pain is an infrequent early symptom • Cancer of sto is advanced before noticed so dismal prognosis (survival rate 10%) • High in Japan, Chile and Eastern Europe- low in US • Increased risk • Atrophic gastric mucosa • Pernicious anemia • 10-20 yrs post gastrectomy for peptic ulcer dz • Lab sign= achlorhydria- absence of hydrochloric acid • Radiographic • Broad spectrum of radiographic appearances • Tumor infiltration • stimulate fibrosis- thick/ narrow, • fixation of stom wall (linitisplastica) • Fundus is least involved • Large irregular polypoid mass • CT is best used to stage gastric CA- Stage 1-4- and demonstration of tumor invasion to intrab organs and liver • Endoscopic US is also used
Pathology of the small bowel • Crohn’s Disease • Small bowel obstruction • Adynamicileus • Intussusception • Malabsorption disorders
Crohn’s Disease • Chronic inflammatory d/o of unknown cause • Involves the TI but also any other part of the GI system • Most common in young adults • Stress and emotional upset go along with relapse • Discontinuous • Diseased segments of bowel with “skip areas” of healthy bowel • Fistula with other bowel or organs • Pain in RLQ- mimic appy- • Blood in stool- congested mucous membranes • Small bowel obst and fistula formation occur in ½ the patients • Rectal fissures/ pereirectal abscess occur in 1/3 • Radiographic • Irregular thickening/ distortion of mucosal folds • Cobbleestone appearance • Skip lesions- normal and abnormal segments of bowel • Fistula- tracts ending into blind abscess cavities- fever/pain – to bladder or vagina
Small Bowel Obstruction • 75% of fibrous adhesions or from previous surgery/ peritonitis • Second is external hernias • Lastly • mechanical- gallstone, intussusception • Intrinsically- neoplastic, inflamm or vascular insufficiency • Radiographic • Distended loops of small bowel with mainly gas and some fluid • All gas proximal to the obstruction is swallowed air • Image the gas/fluid levels • The point of obstruction is always distal to the lowest loop of dilated bowel • Mechanical obst- demonstrate little or no gas in the colon • Bowel proximal to obst contains no gas but instead filled with fluid • With closed loop obst- volbulus and incarcerated hernia- loops going toward and away from thee narrowing become onbstructed
AdynamicIleus • Common disorder of intestinal motor activity • Fluid and gas do not progress normally through nonobstructed small and large bowel • Cause is neural, hormonal and metabolic factors • Perotinitis, meds, electrolyte d/o, metabolic and trauma • Or most patients that have had abdominal surgery • Occurs more often than mechanical bowel obstruction • Signs are abdominal distention and decreased bowel sounds • Radiographic • Retention of large amounts of gas/ fluid in dilated sm/lg bowel- enetire bowel uniformly dilated • Localized ileus- isolated distended loop- area of inflam or TI for appy • Colonic ileus- disproportionate distention of lg bowel or cecum • BE is done to rule out an obstructing lesion
Intussusception • Major cause of bowel obstruction in children (under 6) • Telescoping bowel • Proximal segment of bowel moves distally within the ensheathing outer portion of bowel wall • Can compromise vascular supply- ischemic necrosis • Most commonly at the ileocecal valve • Abrupt onset: severe abd pain, blood in stool and “palpable rt mass” • If treatment is delayed >48 hours- mortality rate increases • Children older than 6 or adults with intussusception, a lead point such as a polypoid lesion can be to blame • Radiographic • Coiled spring of barium • US- pseudokidney or bulls eye
Malabsorption D/ O • Defective absorption of carbohydrates, proteins and fats from the small bowel • Steatorrhea- passage of bulky, foul-smelling, high- fat stools that float. • Radiographic • No detectable bowel changes • Or bowel dilation with normal folds • Or pattern of generalized , irregular, distorted small bowel folds
Pathology of the colon • Appendicitis • Diverticulosis • Divereticulitis • Ulcerative colitis • Crohn’s colitis • Ischemic colitis • IBS • Cancer of the colon • Large bowel obstruction • Volvulus of the colon
Appendicitis • Neck of appendix becomes blocked by fecalith • Post inflam scar that creates closed loop obstruction, creating a breeding ground for bacteria, perforation. • Terminal ileum, cecum, omentum may wall off the appendiceal area so localized abscess develops • Perforation- spilling of fecal material into peritoneum causing peritonitis • Children and adolescents are most common age for it to occur. • Symptoms: severe RLQ pain, low grade fever, slight leukocytosis • Radiographic • Round, oval Ca++ in appendix in 1/3 of patients • iliac fossa, retrocecal appendix • BE avoided for perforation • US with compression is modality of choice- >7mm without compressibility is a positive finding
Diverticulosis • Outpouchings- herniation of mucosa and submucosa through muscular layers- points of weakness in bowel wall • Increases with age • When exerting high pressure to pass stool • Sigmoid colon • No symptoms- but many people of chronic lower abd pain • Flare up with meals, emotions stress and bouts of diarrhea and constipation • Lower GI bleeding, occult blood, higher in elderly • Radiographic • Round out pouchings of barium projecting beyond confines of lumen • Barely visible to 2 cm or more in diameter
Diverticulitis • Complication of diverticular disease of colon • Perforation of a diverticulum • 20% of people with diverticulosis develop acute diverticulitis • Retained fecal material trapped in diverticulum by a narrow opening causes inflammation of the mucosal lining leading to perforation • Common complication is a fistula developing to adjacent organs- bladder, vagina, ureter, or small bowel. • Radiographic • direct/ indirect evidence of diverticular perforation • Extravasation • Spasm of diverticulitis can cause rigidity and narrowing of the colon than simulates annular carcinoma • Diverticulitis- gradual, preserve mucosa detail, tracts or abscess- define from a ca mass.
Ulcerative colitis • One of two major inflammatory bowel diseases • Young adults • Variable in severity- maybe autoimmune • Aggravated by stress • Bloody diarrhea, abd pain, fever, wt loss • Alternating remission and relapse • Fewer than 15%- acute- toxic megacolon and free perforation • Involves only mucosal layer of the colon • Radiographic • Plain radiographs • Large protrusions of hyperplastic mucosa, deep ulcers outlined by intramural gas, loss of haustral markings, no skip areas- instead lead pipe colon- smooth- fine granularity of mucosa • sometimes toxic megacolon- abd pain, tender, tachy, fever , leuko- due to perf- no BE • Begins at retrosigmoid- rectum normal only in 20% • Colon Ca-10x more frequent- first 10 yr small risk- then 20% chance per decade.
Crohn’s Colitis • Disease of the colon • Iedentical to Crohn’s of the small bowel- distinguish from colitis • Proximal colon is frequently involved- rectum spared • Patchy distribution- multiple noncontiguous segments- skip areas • Rectal fissure in ½ pt with Crohn’s- rare in ulcerative colitis • Invovles all layers of GI tract • Radiographic • Found only in colon • Dbl contrast- erosions= punctate collections of barium • thin halo of edema • Pathcy distribution • Deeper / irregrular ulcers create the cobblestone appearance • Fibrotic thickening leads to narrowing and stricture, skip lesions, sinus tracts, fistula • Higher colon Ca risk ( proximal colon)
Ischemic Colitis • Abrupt onset of lower abd pain and rectal bleeding • Diarrhea and abd tenderness is common • > 50 yrs with some prior Cardiovascular dz • Radiographic • Fine superficial ulceration by inflammatory edema of mucosa • Deep penetrating ulcers (pseudopolyps) develop • Thumbprinting (finger like indentions) of the colon margins • In 1 month images return to normal- post collateral circulation • Fibrosis during healing can cause narrowing or stricture • If bloodflow remains ineffecient- acute bowel necrosis and perf can result
IBS • Several conditions that have an alteration in intestinal motility • Functional disorders • Chronic abd pain/ constipation/ intermittent watery diarrhea (without pain) or alternating bouts of constipation and diarrhea • Radiographic • No specific findings • BE to exclude another chronic disorder
Colon Cancer • 3rd leading cause of death from cancer in US • ½ occur in rectum and sigmoid • Disease of older folks- peak 50-70- 2x more in men • High risk- ulcerative colitis and familial polyposis ( hereditary dz of many polyps) • Radiographic • Delay most significant in a poor diagnosis • Arise from preexisting polyps • Irregular, sessile lesions (w/ out stalk) >2 cm= malignant • Smooth, pedunculated (stalk) • Annular ca- apple core- most typical primary colon ca • Arise from flat plaques/ saddle lesions- circumference of colon wall • Tends to infiltrate the wall • Progressive constriction cause colonic obstruction- sigmoid • Ulceration is common • CT virtual colonoscopy for screening- staging or recurrence • Transrectal US staging • PET for distant mets
Large Bowel Obstruction • 70% result from primary colonic cancer • Diverticulitis and volvulus make up the other 30% • Radiographic • Depends on competency of ileocecal valve • Valve competent- obstruction causes large dilated colon with greatly distended thin walled cecum- small bowel gas- colon distal to obstruction is collapsed and free of air • Valve incompetent- distention of gas-filled loops of both colon and small bowel- simulate adynamicileus • Major danger is perforation- cecum > 10 cm
Volvulus of the colon • Twisting of bowel on itself- may lead to intestinal obstruction • Large bowel- involves cecum and sigmoid colon • Sigmoid volvulus in the elderly results from a low fiber diet and constipation • Radiographic • Sigmoid- long redundant loop of sigmoid can twist -form a closed –loop • Inverted U- devoid of haustral markings- sausage or balloon shape • BE shows obstruction at volvulus and distention of rectum- pathognomonic “bird’s beak” sign of barium reaching the site • Water soluble enema banc be therapeutic and resolve the obstruction
Gallbladder • Gallstones (cholelithiasis) • Cholesterol stones (75%) • pigment stones • Famhx, >40 yrs, excess wt, female (4 F’s) • Due to insufficient bile salts/ lecithin in proportion to cholesterol • > hepatic synthesis of cholesterol • Radiographic • Most gstones are radiolucent • 20% contain enough ca++ seen on KUB • US is gold standard for diagnosis- also demonstrate biliary tree • Acute • Obstruction of cystic duct-impacted stone (95%) • Demonstrate distended GB/stones, edema of GB wall and focal tenderness over GB (sonographic Murphy’s sign) • Emphysematous • Rare condition of gas-forming organisms in BG with stasis and ischemia by cystic duct obstruction • Elderly men- poorly controlled diabetes • Radiographic- rim of lucent bubbles or streaks of gas parallel to lumen • Porcelain • Ca++ of GB wall- chronic chole
Liver • Hepatitis • Cirrhosis • HCC • Liver Mets
Liver-hepatitis • Most prevalent inflammatory disease of the liver • Viral, drugs or toxins • HAV- infectious/ transmitted in digestive tract • HBV- contaminated blood/ sex- vaccine • HCV – chronic hepatitis/ cirrhosis/ HCC- blood transfusion/ sex (livtx) • HEV- food or water contaminated by fecal material • Radiographic • Early stages not visible • Disease progresses- starry sky • cirrhosis as macronodules • > echogenicity • Nodular surface • PHTN
Liver- Cirrhosis • Chronic destruction of liver cells • Nodular regeneration of liver parenchyma/ fibrosis • End stage liver dz • Major causes • chronic alcoholism • Toxic effect or malnutrition that accompanies alcoholism • Post necrotic viral hapatitis • Hepatotoxic drugs/ chemicals that destroy liver cells • Disease of the bile ducts • Excessive deposition of iron pigment – hemochromatosis • Radiographic • Accumulation of fat in the liver- see on CT • Liver echotexture is darker with bright portal triads • Coarse echogenicity on US- multhyperechoicmicronodules or macronodules • Nodules and fibrotic change causes PV obstruction (collaterals)- umbilical vein or esophageal varicies • > pressure of liver vessels causes enlargement of the spleeen • Decreased ability to synthesize albumin- cause fluid leak- swelling of extremities • Accumulation of ascites- US best modality • Can no longer detoxify- ammonia causes disorientation- eventually neurological impairment (encephalitis)
HCC • Most commonly occurs in patients with diffuse hepatocellular disease • Alcoholic/ postnecrotic cirrhosis • Symptoms- RUQ discomfort/ wt loss/ hemorrhagic shock • Rupture of tumor or invasion of biliary tree • Radiographic • CT- modality of choice for HCC • Large mass- solitary or small # of lesions • Invade portal and hepatic venous systems • US is used to screen chronic hepatitis B
Liver Mets • Most common malignant tumors involving the liver • CT, US, MRI or nuc med to dx • Radiographic • Well marginated, less dense • MRI shows low signal lesions on T1 and bright on T2- good for non con folks • US and nuc med can see evidence of masses in liver- but less sensitive
Pancreas • Acute pancreatitis • Inflammatory- protein and lipid digesting enzymes begin to self digest • Excessive alcohol consumption, less frequent is gallstone obstruction • First symptom- severe abd pain- radiate to back • Radiographic • Local adynamicileus- jejunum • US and CT- define the degree- alter both size and parenchymalechogenicity • Chronic pancreatitis • Frequent intermittent pancreatic injury creates scar tissue • Chronic alcohol abuse • Pain, malabsorption w/ wt loss and diabetes • Radiographic • CA++ pathognomonic finding in chronic pancreatitis- 1/3 patients • US alteration of echo patteren- enlarged then atriphic • Pseudocyst development
Pancreas contd. • Pseudocyst • Loculated / walled off fluid collections • Inflammation, necrosis and hemorrhage with acute pancreatitis or trauma • Traumatized pancreas continues to release enzymes • Radiographic • US- echo free cystic structure • CT- best delineated after contrast • Pancreatic cancer • Adenocarcinoma 90% • Mets before diagnosed • 60% at the head • Insulinoma- benign at tail • Radiographic • US best screening- especially at Panc head- >2 cm • CT is best for dx tumors in any part of the panc • Obstructive jaundice – tumor at head obstructs the bile duct
Pneumoperitoneum • Free air in the peritoneal cavity • Abdominal pain/ tenderness • Perforation of bowel (peptic ulcer) • Surgical emergency • Less common- abd, gyn, intrathoracic or iatrogenic and no need for OR • Radiographic • Dx of perf of GI tract • Accumulates at domes of diaphragm • Upright or decub best demonstrated
Spleen • Enlargement (splenomegaly) associated with numerous conditions- infection, connective tissue d/o, neoplastic, hematologic, hemolytic anemia and hemoglobinopathies and PHTN • Radiogrpahic • Plain KUB can demonstrate inferior border of an enlarged spleen • Elevate the left diaphragm • Downward displacement of left kidney • Rupture • Caused by trauma • Rapid loss of blood into the abdominal cavity • Immediate surgery • Radiographic • CT is best for blunt trauma- splenic injury