Download
1 / 23
260 likes | 785 Views
Learn how intraosseous infusion works, its indications, contraindications, proper technique, and possible complications. Discover the step-by-step procedure and preparation of IO equipment to ensure safe and efficient use in emergency situations.

E N D
Intraosseous Insertion Gwen Hollaar University of Calgary
Outline • How does it work • Indications and Contraindications • Technique • Complications • Review
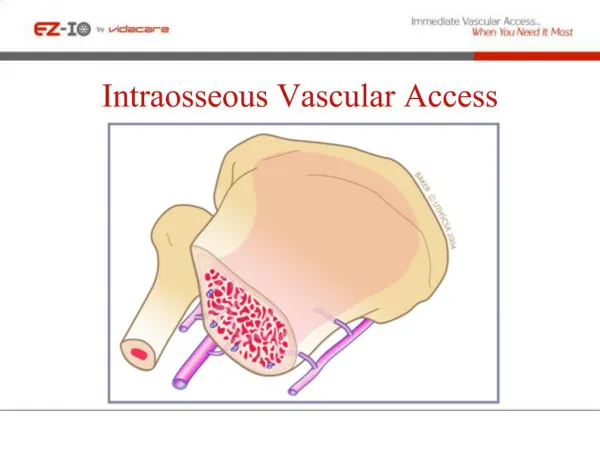
How Does It Work • Bone has two components • Bone cortex • Bone marrow • Bone marrow contains • Developing blood cells • Framework for vascular complex of the medulla • Provides blood supply for bone
How Does It Work • Path of fluids into body blood vessels • Fluid enters venous sinusoids in medullary cavity • Fluid drains into central venous channel • Fluid exits bone cortex through nutrient veins
How Does It Work • Intraosseous (IO) infusion • Can deliver fluids as quickly as IV method • Can administer drugs and blood through IO infusion • Onset and peak drug levels are similar to IV administration
Indications and Contraindications • Indications • EMERGENCY VASCULAR ACCESS when usual methods have failed • Initially recommended in children < 6 years • Now also recognized as useful resuscitation technique for adults
Indications and Contraindications • Absolute Contraindication • Fracture near access site • Relative Contraindications • Cellulitis over insertion site • Bacteremia • Osteoporosis
Technique • Sterile Procedure • Equipment • Sterile gloves • Drape • Alcohol or cleaning solution • IO needle holder • 12 to 20 gauge needle • Gauze • Tubing • 10 or 20 cc syringe or IV bag
Technique: Intraosseous Needle Holder Designed and made by Richard Near rbn@nearmfg.com
Technique • Choice of needle: • Children • < 18 months • 16, 18, or 20 gauge needle • 18 months to 6 years • 12, 14, 16 gauge needle • Older children and adults • 12 or 14 gauge needle
Technique • Usually use proximal tibia because easy to landmark • Need to be distal to growth plate in children • Landmark • Palpate tibial tuberosity • Move distal 2 cm and slightly medial • Relatively flat area
Technique • Place small towel behind knee • Restrain leg • Use local anesthetic in subcutaneous tissue and periosteum if patient conscious as the procedure is painful • Put on gloves / Drape area / Sterile technique • Load needle onto IO needle holder
Technique foot knee • Landmark and insert needle angled to 10-15º caudally -- to avoid injury to growth plate • Insert through skin until you feel bone • Begin to twist and push - Keep index finger down on IO holder to prevent plunging in • You will feel a ‘pop’ when you reach marrow • Immediately flush small amount of sterile fluid through needle to dislodge ‘bone plug’
Technique • Confirm proper location of needle before starting infusion • Needle should stand on its own without support if it is through bone cortex • Aspirate blood or marrow • 5-10 ml bolus should enter with little resistance and with no extravasation • If you make a hole in the cortex, do not put another hole in the cortex of the same bone as this will result in possible fluid extravasation into the soft tissue
Technique • Attach stopcock or syringe or IV tubing • Tape gauze pads around needle to stabilize it • Should use IO access for resuscitation and replace with conventional IV line when resuscitation is completed • IO lines should not be used for a prolonged period of time to minimize risk of osteomyelitis
Technique • Use syringe to give fluid bolus • If needle is attached to IV tubing, you need pressure bag or pump to infuse at a rapid rate • Use isotonic solution (normal saline) • For resuscitation in children: 20 ml / kg
Possible Complication • Extravasation of fluid into subcutaneous tissue • Most common complication • Caused by: • Misplaced needle • Multiple attempts (put other holes in bone) • Enlargement of IO hole from needle movement • May result in: • Subcutaneous tissue or muscle necrosis • Compartment syndrome
Possible Complications • Osteomyelitis • Incidence in children is 0.6% • Risk increased if: • Prolonged use of IO needle • Pre-existing bacteremia • Use of hypertonic saline • Other rare complications • Fracture at IO site • Compartment syndrome • Cellulitis or local abscess
Preparation of IO Holder • Needs to be cleaned and sterilized after each use • Can be used and cleaned like all other surgical instruments because it is stainless steel • Method • Cleaning • Sterilization
Preparation of IO Holder • Cleaning • Use scrub brush • Decreases possible pieces of blood and tissue that prevents heat or chemical sterilization
Preparation of IO Holder • Chemical Sterilization • Undiluted bleach or 1:1 bleach dilution • Kills bacteria, virus, fungus, TB (not bacterial spores) • Needs 1 hour contact, then rinse with sterile water • 2% glutaraldehyde • Needs 6-10 hour contact, then rinse with sterile water • Heat Sterilization • Autoclave • Unwrapped at 124ºC for 15 minutes • Kills bacteria, virus, fungus, TB, and bacterial spores • Steam Sterilization • Wrapped at 121ºC for 30 minutes
Review • Important way to gain emergency IV access for resuscitation when other methods have failed • Placement of needle is in flat area medial and distal to tibial tuberosity • Confirm position and stabilize needle • Bolus 20 ml / kg in children • Replace with conventional IV line when resuscitation completed
References • Intraosseous Infusion • Brian LaRocco, Henry Wang • Prehospital Emergency Care 2003;7:280-285 • Clinical Review: Vascular Access for fluid infusion in children • Nikolaus Haas • Critical Care 2004;8(6):478-484