Download
1 / 26
340 likes | 1.27k Views
Intraosseous Needle Insertion. Kalpesh Patel, MD Dept. of Pediatric Emergency Medicine November 22, 2006. Objectives. Understand the history of intraosseous needles (IO) Understand the indications, risks, and benefits of IO needle insertion Learn to perform:

E N D
Intraosseous Needle Insertion Kalpesh Patel, MD Dept. of Pediatric Emergency Medicine November 22, 2006
Objectives • Understand the history of intraosseous needles (IO) • Understand the indications, risks, and benefits of IO needle insertion • Learn to perform: • IO needle insertion at various locations using the manual insertion method • IO needle insertion using new techniques
History • Earliest reference to IO use was in 1922 • First theraputic use in humans was reported in 1934 • Popularized in the 1940’s for rapid access • Used widely until 1950’s when the plastic catheter was devised • Reemerged in mid 80’s for resuscitation where IV access was difficult • Since then, pediatric use has become more accepted • Now used as the standard of care for emergency access in both pediatrics and adults
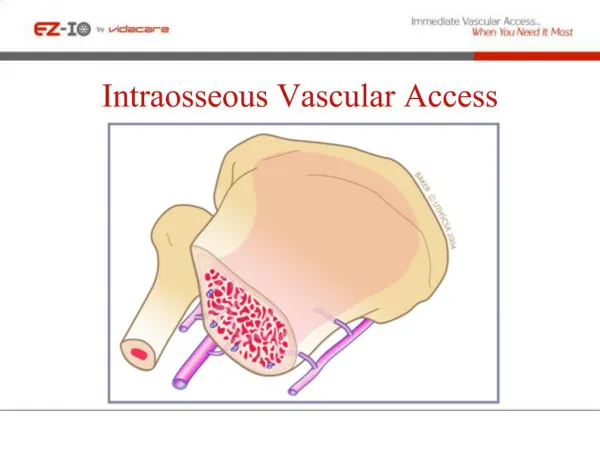
Physiology • The marrow cavity is in continuity with the venous circulation and functions as a non-collapsable venous plexus • Sinusoids serve as transport to the central venous channel exiting as nutrient and emissary veins
Physiology • The onset of action and drug levels during CPR using the IO route are similar to those given IV • Used to infuse fluids, blood products, and drugs • Can take mixed venous blood samples for labs such as crossmatch, bedside tests, etc.
Indications • When vascular access is needed in life-threatening situations • When attempts at standard venous access fail (three attempts or 90 seconds) or in cases where it is likely to fail and speed is of the essence.
Contraindications • Femoral fracture on the ipsilateral side • Do not use fractured bones • Do not use bones with osteomyelitis • Osteogenesis Imperfecta • Osteopetrosis
Types of IO Needles Jamshidi IO Needle Cook IO Needle Sur-Fast IO Screw Tip Needle Illinois Sternal Iliac Needle
Equipment Required • Antiseptic prep solution • Local Anesthetic (optional in the moribund patient) • IO Needles • 18-20 gauge spinal needle can be used as an alternative • In a pinch, any needle can be used, but may get clogged with cortical bone without stylet or trochar • Syringe • Flush solution • Gauze pads and tape
Locations of Insertion • 3 most common locations: • Proximal Tibia • Medial side, 1-2 cm below and avoiding the tibial tuberosity
Locations of Insertion • Distal Femur • Femur is triangular shaped. Insert needle 1-2 cm proximal to the superior border of patella and medial or lateral to anterior ridge • Distal Tibia • 1-2 cm proximal to the medial malleolus in the center of the bone
Locations of Insertion • In older children and adults: • Iliac crests, preferably Anterior Superior Iliac Spine • Sternum
Technique for Manual Insertion • Prep the site • Inject 1-3 ml of lidocaine into the skin and down to the periosteum (optional when time does not permit this) • Grasp needle in dominant hand and place it on the site with the needle pointing away from the joint • Pinch needle with thumb and forefinger and allow the hub to rest in the palm of your hand • DO NOT PLACE YOUR OTHER HAND BENEATH THE SITE
Technique for Manual Insertion • Use firm downward pressure and rotate the needle back and forth • Feel for a sudden decrease in resistance or a popping sound and advance the needle a few millimeters • Remove the trochar or stylet and aspirate marrow
Technique for Manual Insertion • Infuse fluid to determine ease of flow and no extravasation in to soft tissues around the insertion site • Secure the needle with goal post taping to allow visualization of the site • If the needle fails, then insert into a new bone because fluid will leak from the failed site
IO Insertion http://www.cookmedical.com/cc/datasheetMedia.do?mediaId=1528&id=1347
Complications • Through and through penetration • Extravasation of fluids or medications into subcutaneous tissue • Compartment syndrome • Subcutaneous abscess/skin necrosis • Osteomyelitis • When an aseptic technique is used, the incidence of osteomyelitis is less than 1% • Bacteremia • Epiphyseal injury and fracture (especially in neonates) • Fat Embolus • Bent needle • Complications are reported to occur in <1% of cases
New Methods • F.A.S.T -1 system • Bone Injection Gun (BIG) • EZ-IO Drill
F.A.S.T. -1 Sternal Intraosseous Device • First Access for Shock and Trauma • Created for insertion into manubrium of adult sternum • May be used in older children • http://www.pyng.com/movies/iousemovie.html
Bone Injection Gun • Spring loaded catheter injected into place at a preset depth • Comes in Adult and Pediatric sizes • Establishes access within 1 minute
BIG, The Movie http://www.ps-med.com/big/description_big01.html
EZ-IO • A battery powered electric drill which places the needle quickly into place
EZ-IO Insertion http://www.vidacare.com/Products/index_4_29.html
Aftercare • IO’s are emergency lines and every effort should be made to place an intravenous line after initial resuscitation • IO’s should ideally be removed within 6-12 hours • All IO’s will eventually start to leak • IO’s can stay in for up to 48-72 hours, but after 24 hours the risk of osteomyelitis increases dramatically
Summary • IO’s are essentially equivalent to IV access • Should be used for emergency access • Many types of needles exist, but Jamshidi style is preferred by most users • Preferred insertion sites include proximal or distal tibia, or distal femur, but in older children, iliac crests and sternum can be considered • New devices are emerging, but are not standard of care in pediatrics yet