Download
1 / 30
330 likes | 746 Views
THERAPEUTIC PLASMA EXCHANGE OUR EXPERIENCE AT SALEM. Dr. Aswin Kumar. S II year M.D., Immunohematology & Blood Transfusion Vinayaka Mission Medical College, Salem. INTRODUCTION .

E N D
THERAPEUTIC PLASMA EXCHANGE OUR EXPERIENCE AT SALEM Dr. Aswin Kumar. S II year M.D., Immunohematology & Blood Transfusion Vinayaka Mission Medical College, Salem
INTRODUCTION • APHERESIS, The Greek word ‘Pheresis’ meaning “to take away,” involves the selective removal of blood constituents from donors or patients. Whole blood
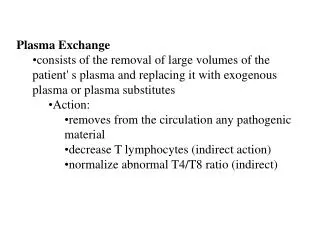
INTRODUCTION Therapeutic plasma exchange (TPE),is an extracorporeal blood purification technique used to remove large molecular weight substance like • Pathogenic autoantibodies(e.g. Myasthenia Gravis: autoantibody) • Cryoglobulins or other abnormal plasma proteins(e.g. Waldenstorm'smacroglobulinemia) • Immune complexes(e.g. Goodpasture's syndrome)
INDICATIONS Approximately 300,000 plasma exchangeprocedures are performed worldwide for various indications like • Neurological - GBS,MG • Renal -Good pasture syndrome • Hematological-TTP, Sickle cell crisis • Dermatology –Pemphigusvulgaris • Toxins-Amanita phalloids, OPC
OUR EXPERIENCE • We started TPE in Jan 2011 till date we have done 110 procedureson 36 patients
CASE DISTRIBUTION Total no of patients : 36
GENDER DISTRIBUTION Total patients = 36
PROCEDURE • Instrumentation : Hemonitics cell separator (MCS+) • Done at : ICU under the supervision of emergency physician • IV access : Central venous catheter (femoral or internal jugular vein) • Anticoagulant : Acid citrate dextrose (ACD) anticoagulant is used in 1:16 ratio
KEEP AN EYE ON • Pulse • Blood pressure • Urine output • Blood flow • Signs of citrate toxicity
VOLUME OF PLASMA EXCHANGE Formula: The volume of plasma to be exchanged is determined by patients estimated plasma volume (EPV) and hematocrit (hct) EPV = 0.07 x weight(kg) X (1-hct) in liters
Efficiency of removal is greatest early in the procedure and diminishes progressively during the exchange.
NUMBER OF PROCEDURES • Neuro-immunological cases Approximately 5 procedures were done on alternate days • Paraquat poisoning Single large volume exchange (1-1.5 plasma volume exchange)
REPLACEMENT FLUIDS • Fresh frozen plasma (30 – 40%) • Colloids(6% hydroxyethyl starch) (30%) • Crystalloids (30%)
ADVERSE REACTIONS 27 9
ADVERSE REACTIONS 1 patient 2 patients
SIGNS OF RECOVERY In Neuro-immnological cases recovery is assessed by • Recovery from assisted ventilator support • Improvement in muscle power and early mobilization
MORTALITY IN PARAQUAT POISONING 8 patients
CONCLUSION The efficacy of plasma exchange in various clinical indications are categorized as follows Category I – Standard acceptable therapy Category II – Sufficient evidence to suggest efficacy usually as adjunctive therapy Category III – inconclusive evidence of efficacy or uncertain risk/benefit ratio Category IV – Lack of efficacy in controlled trials
CATEGORY - I INDICATIONS(first line therapy ) Neurological: • GuillainBarresynd • Myasthenia Gravis • CIDP • Demyelinatingpolyneuropathy with IgG & IgA Hematological: • TTP • Sickle cell crisis • ABO mismatch Marrow transplant • Cryoglobinemia Others: • Cutaneous T cell Lymphoma • Good pasteursynd • Hypercholestrolemia • Phytanic acid storage disease • Amanita phalloides poisoning
CATEGORY - II INDICATIONS Neurological: • Lambert -Eaton synd • Acute CNS inflamatorydemyelinating disease • Sydenham’s chorea • PANDAS • Refsum’s diseases Hematological: • ITP • Maternal-fetal Rh incompatability • Coagulation factors inhibitors Renal & Others: • RPGN • Acute renal failure due to cast nephropathy • Graves disease • Digitalis toxicity • Pemphigusvulgaris • Bullous pemphigoid • Toxic epidermonecrolysis
CONCLUSION • TPEs are successfully performed worldwide but implementation of plasma exchange in our country is still lacking • The risks and complications associated with this procedure are minimal and manageable • Utilization of this procedure in large scale will prove beneficiary to patients
CONCLUSION Therapeutic plasma exchange is • Safe • Cost effective and • Efficacious when performed with expertise in appropriate indications TPE