Download
1 / 2
20 likes | 137 Views
ELIMINATING COVERED SELF-EXPANDING STENT MIGRATION WITH A NOVEL FIXATION PROCEDURE Calvin Lyons, MD, Min P. Kim, MD, Shanda H. Blackmon, MD, MPH Division of Thoracic Surgery, Department of Surgery The Methodist Hospital, Houston, Texas. Weill Cornell Medical College. TECHNIQUE:

E N D
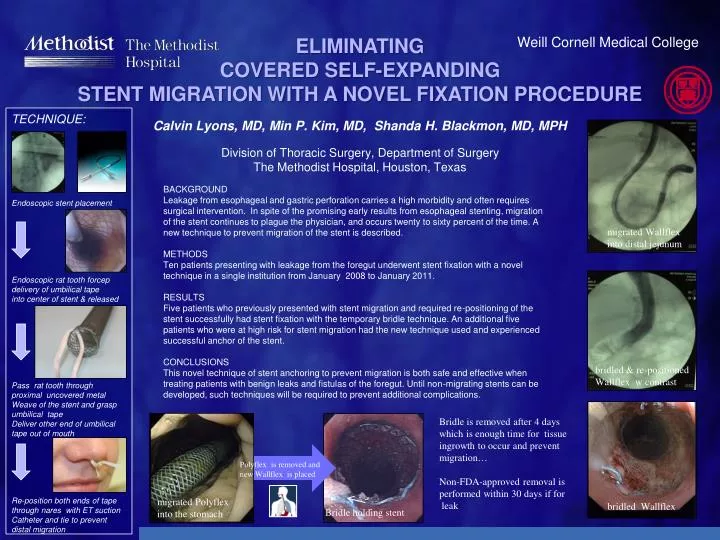
ELIMINATING COVERED SELF-EXPANDING STENT MIGRATION WITH A NOVEL FIXATION PROCEDURECalvin Lyons, MD, Min P. Kim, MD, Shanda H. Blackmon, MD, MPH Division of Thoracic Surgery, Department of Surgery The Methodist Hospital, Houston, Texas Weill Cornell Medical College TECHNIQUE: Endoscopic stent placement Endoscopic rat tooth forcep delivery of umbilical tape into center of stent & released Pass rat tooth through proximal uncovered metal Weave of the stent and grasp umbilical tape Deliver other end of umbilical tape out of mouth Re-position both ends of tape through nares with ET suction Catheter and tie to prevent distal migration BACKGROUND Leakage from esophageal and gastric perforation carries a high morbidity and often requires surgical intervention. In spite of the promising early results from esophageal stenting, migration of the stent continues to plague the physician, and occurs twenty to sixty percent of the time. A new technique to prevent migration of the stent is described. METHODS Ten patients presenting with leakage from the foregut underwent stent fixation with a novel technique in a single institution from January 2008 to January 2011. RESULTS Five patients who previously presented with stent migration and required re-positioning of the stent successfully had stent fixation with the temporary bridle technique. An additional five patients who were at high risk for stent migration had the new technique used and experienced successful anchor of the stent. CONCLUSIONS This novel technique of stent anchoring to prevent migration is both safe and effective when treating patients with benign leaks and fistulas of the foregut. Until non-migrating stents can be developed, such techniques will be required to prevent additional complications. migrated Wallflex into distal jejunum bridled & re-positioned Wallflex w contrast Bridle is removed after 4 days which is enough time for tissue ingrowth to occur and prevent migration… Non-FDA-approved removal is performed within 30 days if for leak Polyflex is removed and new Wallflex is placed migrated Polyflex into the stomach bridled Wallflex Bridle holding stent
ELIMINATING COVERED SELF-EXPANDING STENT MIGRATION WITH A NOVEL FIXATION PROCEDURECalvin Lyons, MD & Shanda H. Blackmon, MD, MPH Division of Thoracic Surgery, Department of Surgery The Methodist Hospital, Houston, Texas Weill Cornell Medical College TECHNIQUE: Endoscopic stent placement Endoscopic rat tooth forcep delivery of umbilical tape into center of stent & released Pass rat tooth through proximal uncovered metal Weave of the stent and grasp umbilical tape Deliver other end of umbilical tape out of mouth Re-position both ends of tape through nares and tie to prevent distal migration BACKGROUND Leakage from esophageal and gastric perforation carries a high morbidity and often requires surgical intervention. In spite of the promising early results from esophageal stenting, migration of the stent continues to plague the physician, and occurs twenty to sixty percent of the time. A new technique to prevent migration of the stent is described. METHODS Ten patients presenting with leakage from the foregut underwent stent fixation with a novel technique in a single institution from January 2008 to January 2011. RESULTS Five patients who previously presented with stent migration and required re-positioning of the stent successfully had stent fixation with the temporary bridle technique. An additional five patients who were at high risk for stent migration had the new technique used and experienced successful anchor of the stent. CONCLUSIONS This novel technique of stent anchoring to prevent migration is both safe and effective when treating patients with benign leaks and fistulas of the foregut. Until non-migrating stents can be developed, such techniques will be required to prevent additional complications. migrated Wallflex into distal jejunum bridled & re-positioned Wallflex w contrast Bridle is removed after 4 days which is enough time for tissue ingrowth to occur and prevent migration… Non-FDA-approved removal is performed within 30 days if for leak Polyflex is removed and new Wallflex is placed migrated Polyflex into the stomach bridled Wallflex Bridle holding stent