Download

1 / 46
460 likes | 476 Views
Learn about pneumothorax, a condition characterized by the presence of air in the pleural cavity. Explore primary and secondary spontaneous pneumothoraces, iatrogenic causes, clinical features, diagnosis using CXR and CT scans, and management strategies including aspiration and chest drainage. Follow-up care and precautions are also discussed.

E N D
PNEUMOTHORAX ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal
Defined as the presence of air in the pleural cavity Negative intrapleural pressure: ~ 5mm
PNEUMOTHORAX Spontaneous: 1. Primary spontaneous P. 2. Secondary spontaneous P. • Secondary: • Iatrogenic • traumatic
Primary spontaneous pneumothoraces • Do not have overt parenchymal disease • increased shear forces in the apex • commonly are smokers & tall young males • risk much more pronounced in female smokers • Genetic factors - Marfan’s syndrome • Defect of connective tissue
Secondary spontaneous pneumothoraces (SSP) occur in the presence of lung disease • COPD • Tuberculosis • sarcoidosis • cystic fibrosis • malignancy • idiopathic pulmonary fibrosis • Pneumocystis carinii pneumonia [PCP]) in patients with AIDS Sub pleural focus rupturing in pleural cavity
Iatrogenic pneumothorax a complication of medical or surgical procedures. results from • Therapeutic thoracentesis • Positive pressure mechanical ventilation • Pleural biopsy • Central venous catheter insertion • Transbronchial biopsy routine use of ultrasonography guided diagnostic thoracentesis is associated with lower rates of pneumothorax
Broncho pleural fistula Intra pleural pressure(0)
Symptoms: • Sudden onset (usually after a bout of coughing) of • Chest pain • dyspnoea • Asymptomatic when small Signs: • In sever cases low volume pulse with tachycardia • Collapse & signs of peripheral circulatory failure • Cyanosis (See when there is tension pneumothorax) • Vitals are normal in closed & open pneumothorax
Inspection: Dyspnoea with accessory muscles active Tracheal shift may be visible – trail’s sign Fullness of chest on affected side Diminished chest movement
Palpation: • Trachea & medistinum shifted to opposite side • Vocal fremitus – markedly diminished • Diminished expansion of affected hemithorax Percussion: • Hyper resonant note on the affected side • Liver dullness obliterated: right sided pneumothorax • Cardiac dullness shifted to opposite side
Auscultation • Vocal resonance reduced/absent • Breath sounds reduced/absent on affected side • Hamman's sign: refers to a click on auscultation in time with the heart sounds, due to movement of pleural surfaces with a left-sided pneumothorax In open pneumothorax • Amphoric breath sound due to broncho pleural fistula may be heard
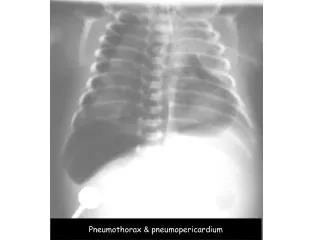
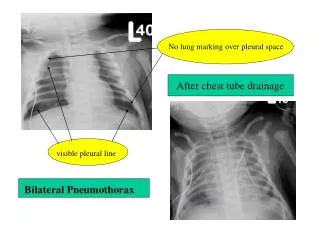
CXR -diagnostic in most cases • visible lung edge and absent lung markings peripherally • increased lucency & hemidiaphragm depression on the affected side • CXR appearance may also show features of underlying lung disease
CT chest may be required • To differentiate pneumothorax from bullous disease • Useful in diagnosing unsuspected pneumothorax following trauma • In looking for evidence of underlying lung disease
Determined by • Degree of breathlessness & lung collapse • Hypoxia • Evidence of haemodynamic compromise • Presence and severity of any underlying lung disease • Pneumothorax size
Severe breathlessness out of proportion to pneumothorax size may be a feature of tension pneumothorax • Secondary pneumothorax has a significant mortality (10%), and should be managed more aggressively. Treat also the underlying disease
Chest Aspiration Suction apparatus
Aspiration Indications Primary pneumothorax Consider aspiration if • patient breathless and/or • pneumothorax large (rim of air > 2 cm on CXR) Secondary pneumothorax Consider aspiration • patient aged > 50 years (all cases) • with small pneumothorax (rim of air < 2 cm on CXR) • minimal breathlessness
Chest drainage • Associated with significant morbidity and even mortality due to subcutaneous emphysema • not required in the majority of patients with primary spontaneous pneumothorax
Oxygen • All hospitalized patients should receive high flow (10 l/min) inspired oxygen (unless CO2 retention is a problem) • Reduces the partial pressure of nitrogen in blood, encouraging removal of air from the pleural space and speeding up resolution of the pneumothorax
Persistent air leak • Defined as continued bubbling of chest drain 48 hours after insertion In indicates: • Inability of lung to expand after the drainage • Broncho pleural fistula - communication with out side air • Will develop secondary infection and pyopneumothorax until closed by surgery
Out-patient follow-up Repeat CXR to ensure resolution of pneumothorax and normal appearance of underlying lungs Discuss risk of recurrence and emphasize smoking cessation, if appropriate
Patients should not fly for at least 6 weeks. avoid flying for a longer period, e.g. 1 year Advise about flying
Advise NEVER TO DIVE in the future, unless patient has undergone a definitive surgical procedure
Indications for cardiothoracic surgical referral • Second ipsilateral pneumothorax • Bilateral spontaneous pneumothorax • Persistent air leak (>5 -7 days of drainage) • Spontaneous haemothorax • Professions at risk (e.g. pilots, divers) after first pneumothorax
Chemical pleurodesis • As an alternative for surgery specially in case of recurrent pneumothorax • seal the visceral to the parietal pleura to prevent pleural fluid accumulating. (already described previously)
Pneumothorax acts as a one-way valve • Progressive increase in pleural pressure compresses both lungs and mediastinum • Reduced venous return to the heart, leading to hypotension and cardiac arrest • not related to pneumothorax size can occur with very small pneumothoraces in the context of air trapping in the lung from obstructive lung disease
Patients present with • Acute respiratory distress & agitation • Hypotension • Raised jugular venous pressure • Tracheal deviation away from the pneumothorax side • Reduced air entry on affected side • May present with cardiac arrest (pulseless electrical activity) • Acute deterioration in ventilated patients
Management • Give high-flow oxygen • Insert a needle into second intercostal space in midclavicular line on side of pneumothorax • Do not wait for a CXR if cardiac arrest has occurred or the diagnosis is clinically certain • Hissing air confirms diagnosis. Aspirate air until the patient is less distressed • Insert chest drain in mid axillary line afterwards