Download
1 / 39
390 likes | 408 Views
Learn about the global epidemic of obesity, its impact on health, assessment methods like BMI, fat distribution, and genetic factors contributing to obesity. Discover key insights to address obesity.

E N D
Obesity is a disorder of body weight regulatory systems characterized by an accumulation of excess body fat. • In primitive societies, in which daily life required a high level of physical activity and food was only available intermittently, a genetic tendency favoring storage of excess calories as fat had a survival value. • However, the current abundance of food has encouraged Americans to eat more.
This, in combination with reduced activity levels found in industrialized societies, has resulted in a tendency for the sustained deposition of fat. • The prevalence of obesity increases with age. As adiposity has increased so has the risk of developing associated diseases, such as diabetes, hypertension, and cardiovascular disease.
Particularly alarming is the explosion of childhood obesity, which has shown a three fold increase in prevalence over the last two decades. Obesity is not limited to the United States, but rather has increased globally. In fact, by some estimates, there are more obese than undernourished individuals worldwide.
Assessment of Obesity • The amount of body fat is difficult to measure directly, and is usually determined from an indirect measure—the body mass index (BMI)—which has been shown to correlate with the amount of body fat in most individuals. • Notable exceptions are athletes who have large amounts of lean muscle mass.
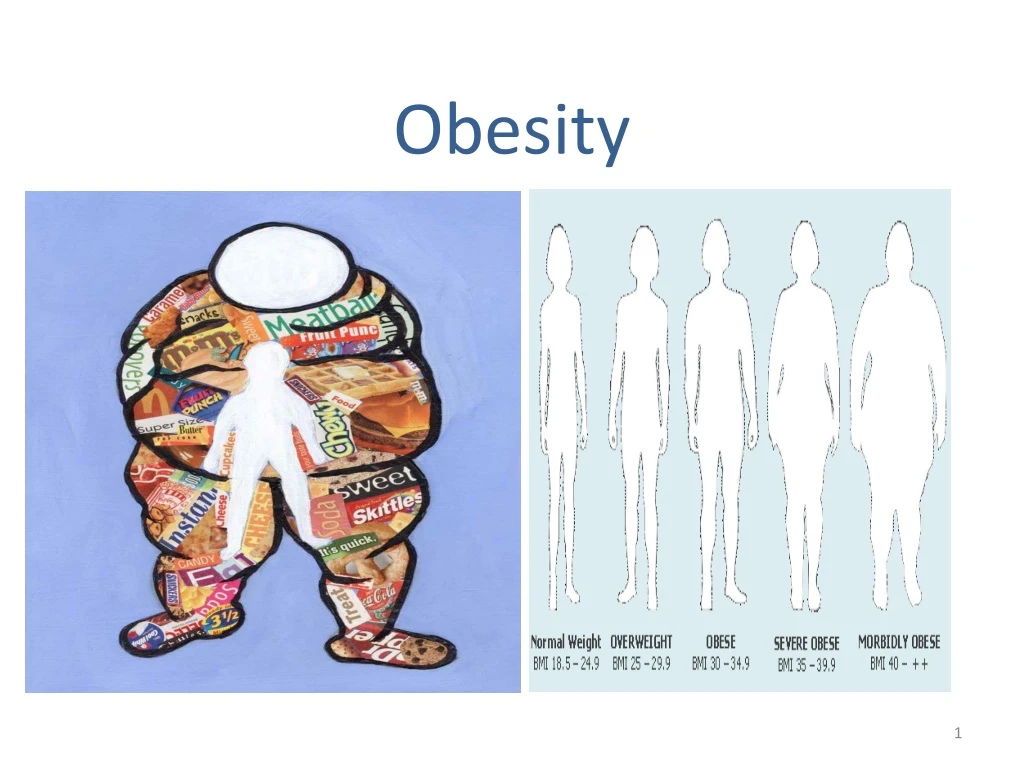
Body mass index • The BMI gives a measure of relative weight, adjusted for height. • The BMI is calculated in both men and women as follows: BMI = (weight in kg)/(height in meters)2 = (weight in lb)/(height in inches)2 × 703 • The healthy range for the BMI is between 19.5 and 25.0. • Individuals with a BMI between 25 and 29.9 are considered overweight, those with a BMI equal to or greater than 30 are defined as obese. • Nearly two thirds of American adults are overweight, and more than 36% are obese.
Anatomic differences in fat deposition Apple-shaped body: • The anatomic distribution of body fat has a major influence on associated health risks. • Excess fat located in the central abdominal area of the body is called android, “apple-shaped,” or upper body obesity, and is associated with a greater risk for hypertension, insulin resistance, diabetes, dyslipidemia, and coronary heart disease. • It is defined as a waist to hip ratio of more than 0.8 for women and more than 1.0 for men.
Pear-shaped Body: • Fat is distributed in the lower extremities around the hips is call gynoid, “pear-shaped,” or lower body obesity. • It is defined as a waist to hip ratio of less than 0.8 for women and less than 1.0 for men. • The pear shape is relatively benign healthwise, and is commonly found in females. • Some experts feel that the waist-to-hip ratio is better than BMI as predictor of myocardial infarction.
Biochemical differences in regional fat depots • The regional types of fat are biochemically different. • Abdominal fat cells are much larger and have a higher rate of fat turnover than lower body fat cells. • The abdominal adipocytes are also hormonally more responsive than fat cells in the legs and buttocks. Because men tend to accumulate the readily mobilizable abdominal fat, they generally lose weight more readily than women do.
Furthermore, substances released from abdominal fat are absorbed via the portal vein and, thus, have direct access to the liver. • Fatty acids taken up by the liver may lead to insulin resistance and increased synthesis of triacylglycerols, which are released as very-low-density lipoprotein (VLDL). • By contrast, free fatty acids from gluteal fat enter the general circulation, and have no preferential action on hepatic metabolism.
Number of fat cells • When triacylglycerols are deposited in adipocytes, the cells initially show a modest increase in size. • However, the ability of a fat cell to expand is limited, and when its maximal size is reached, it divides. • Most obesity is, therefore, thought to involve an increase in both the number and size of adipocytes. • Fat cells, once gained, are never lost.
Thus, when an obese individual loses weight, the size of the fat cells is reduced, but the number of fat cells is not affected. • An obese individual, with increased numbers of adipocytes, will have to reduce the size of those fat cells in order to normalize fat stores. • These individuals will be in the doubly abnormal state of having too many, too small fat cells.
Genetic contributions to obesity • There is a widely held belief that obesity is a result of uncontrolled, gluttonous eating behavior • However it is now evident that genetic mechanisms play a major role in determining body weight, rather than a lack of willpower. • For example, obesity is often observed clustered in families. If both parents are obese, there is a 70–80% chance of the children being obese. In contrast, only 9% of children were fat when both parents were lean.
The inheritance of obesity is not a result of a defect in a single gene. Rather, obesity behaves as a complex polygenic disease involving interactions between multiple genes and the environment. • The importance of genetics as a determinant of obesity is also indicated by the observation that children who are adopted usually show a body weight that correlates with their biologic rather than adoptive parents.
Furthermore, identical twins have very similar BMI, whether reared together or apart, and their BMI are more similar than those of nonidentical, dizygotic twins.
Environmental and behavioral contributions • The epidemic of obesity occurring over the last decade cannot be explained by changes in genetic factors, which are stable on this short time scale. • Clearly, environmental factors, such as the ready availability of palatable, energy-dense foods, play a role in the increased prevalence of obesity.
Furthermore, sedentary lifestyles, encouraged by TV watching, automobiles, computer usage, and energy-sparing devices in the workplace and at home, decrease physical activity and enhance the tendency to gain weight. • The importance of lifestyle in the development of obesity is reinforced by the observation that when Japanese or Chinese populations migrate to the United States, their BMI increases.
For example, men in Japan (aged 46–49 years) are lean, with an average BMI of 20, whereas Japanese men of the same age living in California are heavier, with an average BMI of 24. • Eating behaviors, such as snacking, portion size, variety of foods consumed, an individual's unique food preferences, and the number of people with whom one eats also influence food consumption and the tendency toward obesity.
Molecules that Influence Obesity • Obesity results when energy intake exceeds energy expenditure. • However, unraveling the mechanism underlying this imbalance involves a complex interaction of biochemical, neurologic, environmental, and psychologic factors. • For example, appetite is influenced by neural signals, circulating hormones, and metabolites—that impinge on the hypothalamus.
These diverse signals prompt release of hypothalamic peptides, and activate outgoing, or efferent, neural signals. Some important afferent signaling molecules regulating appetite and energy consumption include: 1. Hormones of adipose tissue 2. Other hormones influencing obesity
Hormones of adipose tissue • Leptin: • The most well-known mouse gene, named ob (for obesity), leads to severe hereditary obesity in mice. • It has been identified and cloned. In one strain of fat mice, the gene was completely absent, indicating that the gene's protein product is required to keep the animals' weight under control.
The product of the ob gene is a hormone called leptin. Leptin is produced proportionally to the adipose mass and, thus, informs the brain of the fat store level. • It is secreted by fat cells, and acts on the hypothalamus of the brain to regulate the amount of body fat through the control of appetite and energy expenditure.
Leptin's secretion is suppressed by depletion of fat stores (starvation) and enhanced by expansion of fat stores (well-fed state). • Daily injection of leptin causes overweight mice to lose weight and maintain weight loss. • The protein also causes weight loss in mice that are not obese. • In humans, leptin increases the metabolic rate and decreases appetite.
However, plasma leptin in obese humans is usually normal for their fat mass, suggesting that resistance to leptin, rather than its deficiency, occurs in human obesity. Adiponectin & Resistin • Hormones released by adipose tissue may mediate insulin resistance observed in obesity.
Other hormones influencing obesity • Ghrelin, a peptide secreted primarily by the stomach, is the only known appetite-stimulating hormone. • Injection of ghrelin increases short-term food intake in rodents, and may decrease energy expenditure and fat catabolism. • Peptides, such as cholecystokinin, released from the gut following ingestion of a meal can act as satiety signals to the brain. Insulin not only influences metabolism, but also promotes decreased energy intake.
Metabolic Changes Observed in Obesity • The metabolic abnormalities of obesity reflect molecular signals originating from the increased mass of adipocytes. The predominant effects of obesity include dyslipidemias, glucose intolerance, and insulin resistance, expressed primarily in the liver, muscle, and adipose tissue.
A. Metabolic syndrome • Abdominal obesity is associated with a threatening combination of metabolic abnormalities that includes: - glucose intolerance, - insulin resistance, - hyperinsulinemia, - dyslipidemia (low high-density lipoprotein (HDL) and elevated VLDL), and hypertension.
This clustering of metabolic abnormalities has been referred to as the metabolic syndrome, the insulin resistance syndrome, or syndrome X. • Individuals with this syndrome have a significantly increased risk for developing diabetes mellitus and cardiovascular disorders. For example, men with the syndrome are three to four times more likely to die of cardiovascular disease.
B. Dyslipidemia • Insulin resistance in obese individuals leads to increased production of insulin in an effort by the body to maintain blood glucose levels. • Insulin resistance in adipose tissue causes increased activity of hormone-sensitive lipase, resulting in increased levels of circulating fatty acids. • These fatty acids are carried to the liver and converted to triacylglycerol and cholesterol. • Excess triacylglycerol and cholesterol are released as VLDL, resulting in elevated serum triacylglycerols. Concomitantly, HDL levels are decreased.
Obesity and Health • Obesity is correlated with an increased risk of death, and is a risk factor for a number of chronic conditions, including: • adult onset diabetes, • hypercholesterolemia, • high plasma triacylglycerols, • hypertension, • heart disease, • some cancers, • gallstones, • arthritis, and • gout.
The relationship between obesity and associated morbidities is stronger among individuals younger than 55 years. • After age 74, there is no longer an association between increased BMI and mortality. • Weight loss in obese individuals leads to decreased blood pressure, serum triacylglycerols, and blood glucose levels. HDL levels increase.
Mortality decreases (particularly deaths due to cancer). • Some obesity experts suggest that moderately overweight and otherwise healthy individuals should not obsess about weight loss, but rather should direct their energies to a healthier lifestyle, particularly including some exercise in their weekly routine.
Weight Reduction • The goals of weight management in the obese patient are: • First to induce a negative energy balance to reduce body weight, that is, decrease caloric intake and/or increase energy expenditure. • The second aim is to maintain a lower body weight over the longer term.
A. Physical activity • An increase in physical activity can create an energy deficit, and is an important component of weight loss treatments. • In addition, physical activity increases cardiorespiratory fitness and reduces the risk of cardiovascular disease, independent of weight loss. • Persons who combine caloric restriction and exercise with behavioral treatment may expect to lose about 5–10% of preintervention body weight over a period of 4–6 months. Exercise is an essential component of maintaining weight reduction.
B. Caloric restriction • Dieting is the most commonly practiced approach to weight control. • Since 1 pound of adipose tissue corresponds to approximately 3,500 kcal, one can estimate the effect of caloric restriction on the reduction in adipose tissue. • Caloric restriction is ineffective over the long term for many individuals. • More than 90% of people who attempt to lose weight regain the lost weight when dietary intervention is suspended.
Nonetheless, it is important to recognize that, although few individuals will reach their ideal weight with treatment, • weight losses of 10% of body weight over a 6-month period often reduce blood pressure and lipid levels, and enhance control of Type 2 diabetes. • The health benefits of relatively small weight losses should, therefore, be emphasized to the the patient.
C. Pharmacologic and surgical treatment • Two weight-loss medications are currently approved by the U.S. Food and Drug Administration for use in adults who have a BMI of 30 or higher. • The first, sibutramine, is an appetite suppressant that inhibits the reuptake of both serotonin and norepinephrine. • The second, orlistat, is a lipase inhibitor that inhibits gastric and pancreatic lipases, thus decreasing the breakdown of dietary fat into smaller molecules.
Surgical procedures designed to reduce food consumption are an option for the severely obese patient who has not responded to other treatments. • Surgery produces greater and more sustained weight loss than dietary or pharmacologic therapy, but has substantial risks for complications.