Download
1 / 1
10 likes | 26 Views
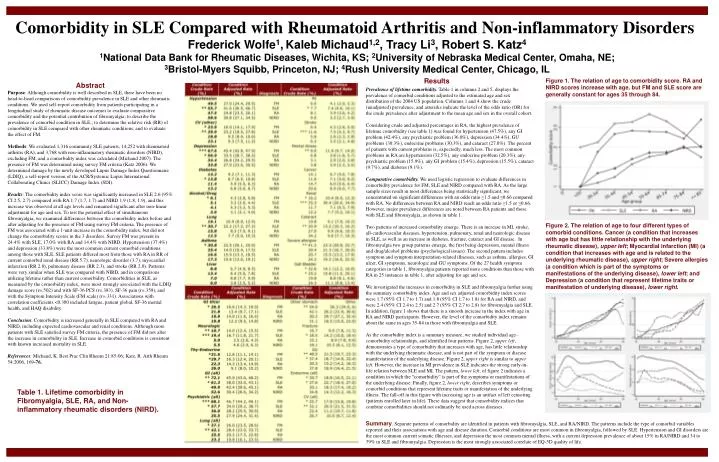
This study compares comorbidity prevalence in systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and non-inflammatory rheumatic disorders (NIRD), and evaluates the impact of fibromyalgia. Results show increased comorbidity in SLE compared to RA and NIRD. The presence of fibromyalgia did not affect the comorbidity scores.

E N D
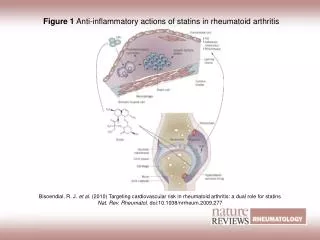
Comorbidity in SLE Compared with Rheumatoid Arthritis and Non-inflammatory Disorders Frederick Wolfe1,Kaleb Michaud1,2, Tracy Li3, Robert S. Katz4 1National Data Bank for Rheumatic Diseases, Wichita, KS; 2University of Nebraska Medical Center, Omaha, NE; 3Bristol-Myers Squibb, Princeton, NJ; 4Rush University Medical Center, Chicago, IL Results Figure 1. The relation of age to comorbidity score. RA and NIRD scores increase with age, but FM and SLE score are generally constant for ages 35 through 84. Abstract Purpose: Although comorbidity is well described in SLE, there have been no head-to-head comparisons of comorbidity prevalence in SLE and other rheumatic conditions. We used self-report comorbidity from patients participating in a longitudinal study of rheumatic disease outcomes to evaluate comparative comorbidity and the potential contribution of fibromyalgia; to describe the prevalence of comorbid condition in SLE,; to determine the relative risk (RR) of comorbidity in SLE compared with other rheumatic conditions; and to evaluate the effect of FM. Methods: We evaluated 1,316 community SLE patients, 14,252 with rheumatoid arthritis (RA), and 3,768 with non-inflammatory rheumatic disorders (NIRD), excluding FM, and a comorbidity index was calculated (Michaud 2007). The presence of FM was determined using survey FM criteria (Katz 2006). We determined damage by the newly developed Lupus Damage Index Questionnaire (LDIQ), a self-report version of the ACR/Systemic Lupus International Collaborating Clinics (SLICC) Damage Index (SDI). Results: The comorbidity index score was significantly increased in SLE 2.6 (95% CI 2.5, 2.7) compared with RA 1.7 (1.7, 1.7) and NIRD 1.9 (1.8, 1.9), and this increase was observed at all age levels and remained significant after non-linear adjustment for age and sex. To test the potential effect of simultaneous fibromyalgia, we examined differences between the comorbidity index before and after adjusting for the presence of FM using survey FM criteria. The presence of FM was associated with a 1-unit increase in the comorbidity index, but did not change the comorbidity scores in the 3 disorders. Survey FM was present in 24.4% with SLE, 17.0% with RA and 14.4% with NIRD. Hypertension (37.4%) and depression (33.8%) were the most common current comorbid conditions among those with SLE. SLE patients differed most from those with RA in RR of current comorbid renal disease (RR 5.7), neurologic disorder (3.7), myocardial infarction (RR 2.8), pulmonary disease (RR 2.3), and stroke (RR 2.0). Patterns were very similar when SLE was compared with NIRD, and in comparisons utilizing lifetime rather than current comorbidity. Comorbidities in SLE, as measured by the comorbidity index, were most strongly associated with the LDIQ damage score (r=.502) and with SF-36 PCS (r=.383), SF-36 pain (r=.359), and with the Symptom Intensity Scale (FM scale) (r=.331). Associations with correlation coefficients <0.300 included fatigue, patient global, SF-36 mental health, and HAQ disability. Conclusion: Comorbidity is increased generally in SLE compared with RA and NIRD, including expected cardiovascular and renal conditions. Although more patients with SLE satisfied survey FM criteria, the presence of FM did not alter the increase in comorbidity in SLE. Increase in comorbid conditions is consistent with known increased mortality in SLE. References: Michaud, K. Best Prac Clin Rheum 21:85-06; Katz, R. Arth Rheum 54:2006, 169-76. Prevalence of lifetime comorbidity. Table 1 in columns 2 and 5, displays the prevalence of comorbid conditions adjusted to the estimated age and sex distribution of the 2004 US population. Columns 1 and 4 show the crude (unadjusted) prevalence, and asterisks indicate the level of the odds ratio (OR) for the crude prevalence after adjustment to the mean age and sex in the overall cohort. Considering crude and adjusted percentages in RA, the highest prevalence of lifetime comorbidity (see table 1) was found for hypertension (47.5%), any GI problem (42.4%), any psychiatric problem (36.0%), depression (34.4%), GU problems (30.3%), endocrine problems (30.3%), and cataract (27.0%). The percent of patients with current problems is, expectedly, much less. The most common problems in RA are hypertension (32.5%), any endocrine problem (20.3%), any psychiatric problem (15.9%), any GI problem (15.4%), depression (15.5%), cataract (9.7%), and diabetes (9.1%). Comparative comorbidity. We used logistic regression to evaluate differences in comorbidity prevalence for FM, SLE and NIRD compared with RA. As the large sample sizes result in most differences being statistically significant, we concentrated on significant differences with an odds ratio ≥1.5 and ≤0.66 compared with RA. No differences between RA and NIRD reach an odds ratio ≥1.5 or ≤0.66. However, major prevalence differences are noted between RA patients and those with SLE and fibromyalgia, as shown in table 1. Two patterns of increased comorbidity emerge. There is an increase in MI, stroke, all-cardiovascular diseases, hypertension, pulmonary, renal and neurologic disease in SLE, as well as an increase in diabetes, fracture, cataract and GI disease. In fibromyalgia two group patterns emerge, the first being depression, mental illness and drug/alcohol problems (psychological issues). The second pattern includes symptom and symptom interpretation-related illnesses, such as asthma, allergies, GI ulcer, GI symptoms, neurologic and GU symptoms. Of the 27 health symptom categories in table 1, fibromyalgia patients reported more conditions than those with RA in 25 instances in table 1, after adjusting for age and sex. We investigated the increases in comorbidity in SLE and fibromyalgia further using the summary comorbidity index. Age and sex adjusted comorbidity index scores were 1.7 (95% CI 1.7 to 1.7) and 1.8 (95% CI 1.7 to 1.8) for RA and NIRD, and were 2.4 (95% CI 2.4 to 2.5) and 2.7 (95% CI 2.7 to 2.8) for fibromyalgia and SLE. In addition, figure 1 shows that there is a smooth increase in the index with age in RA and NIRD participants. However, the level of the comorbidity index remains about the same in ages 35-84 in those with fibromyalgia and SLE. As the comorbidity index is a summary measure, we studied individual age–comorbidity relationships, and identified four patterns. Figure 2, upper left, demonstrates a type of comorbidity that increases with age, has little relationship with the underlying rheumatic disease, and is not part of the symptom or disease manifestation of the underlying disease. Figure 2, upper right is similar to upper left. However, the increase in MI prevalence in SLE indicates the strong early-in-life relation between SLE and MI. The pattern, lower left, of figure 2 indicates a condition in which the “comorbidity” is part of the symptoms or manifestations of the underlying disease. Finally, figure 2, lower right, describes symptoms or comorbid conditions that represent lifetime traits or manifestation of the underlying illness. The fall-off in this figure with increasing age is an artifact of left censoring (patients enrolled later in life). These data suggest that comorbidity indices that combine comorbidities should not ordinarily be used across diseases. Figure 2. The relation of age to four different types of comorbid conditions. Cancer (a condition that increases with age but has little relationship with the underlying rheumatic disease), upper left; Myocardial infarction (MI) (a condition that increases with age and is related to the underlying rheumatic disease), upper right; Severe allergies (a condition which is part of the symptoms or manifestations of the underlying disease), lower left; and Depression (a condition that represent lifetime traits or manifestation of underlying disease), lower right. Table 1. Lifetime comorbidity in Fibromyalgia, SLE, RA, and Non-inflammatory rheumatic disorders (NIRD). Summary. Separate patterns of comorbidity are identified in patients with fibromyalgia, SLE, and RA/NIRD. The patterns include the type of comorbid variables reported and their associations with age and disease duration. Comorbid conditions are most common in fibromyalgia, followed by SLE. Hypertension and GI disorders are the most common current somatic illnesses, and depression the most common mental illness, with a current depression prevalence of about 15% in RA/NIRD and 34 to 39% in SLE and fibromyalgia. Depression is the most strongly associated correlate of EQ-5D quality of life.