Download

1 / 19
190 likes | 249 Views
Dynamometer Training 5/15/2013. Rationale Dynamometer vs Manual Muscle Testing Anatomy 101 Practice. Agenda . Muscle strength is correlated to function, work productivity, and general quality of life. Muscle function becomes compromised: (1) with age,

E N D
Dynamometer Training 5/15/2013
Rationale • Dynamometer vs Manual Muscle Testing • Anatomy 101 • Practice Agenda
Muscle strength is correlated to function, work productivity, and general quality of life. Muscle function becomes compromised: (1) with age, (2) when associated with a skeletal impairment, (3) as a secondary consequence of many disease processes. Iazzo & Dupfree, 2006 • In PACS study can help identify “missed” compartment syndromes Testing Muscle strength
In a word: Subjectivity • Manual Muscle Test: Tester assigns a score to strength of isometric movement. Results often vary with experience of examiner and with clinical judgment • Dynamometers: Provides precise readouts of the resistive force the muscle works against; good inter rater and test-retest reliability Iazzo & Dupfree, 2006 Dynamometers vs MMT
6 month follow up • Test each muscle on each limb 3 times. Record all 3 values • Knee flexion/extension, • Ankle dorsiflexion, • Subtalar joint inversion/eversion • Heel raise tests (no dynamometer) Use of dynamometers in Pacs study
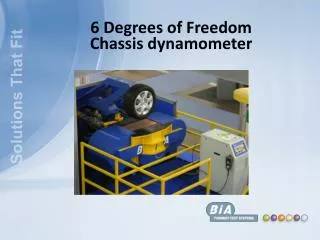
MicroFET2 • This is the equipment we will be using • Out of the box Calibrated • Re-calibration is recommended annually Use of dynamometers in Pacs study
Subject seated • Hips flexed to 90 degrees; hands folded on chest. • Dynamometer Placement: 10 cm Anatomy – Knee EXTENSION superior to the lateral malleolus (0uter ankle)with the dynamometer against the anterior tibia (shin bone).
Positioning – Knee Extension Subject on edge of plinth, arms crossed. Extend leg to raise foot Placement 10 cm above ankle, on shin
Subject prone • Hips at flat, testing knee flexed to 90 degrees; hands resting under head Anatomy – Knee FLEXION • Dynamometer Placement: 10 cm superior to the lateral malleolus (0uter ankle)with the dynamometer placed at center of calf.
Positioning – Knee Flexion Subject prone, hips neutral, testing leg at 90 arms under head. Pull foot toward hips Placement 10 cm above ankle, at center of calf
Subject supine, heels just off the edge of table and hands on chest • Hips, knees, and ankle in neutral position Anatomy – Ankle dorsiflexion • Dynamometer Placement: Just proximal to the metatarsophalangeal joints (big toe)of the foot.
Positioning – Ankle Dorsiflexion Subject supine, hips knees and ankle neutral Pull toes up. Placement just above the big toe joint
Subject supine, heels just off the edge of table and hands on chest • Hips, knees, and ankle in neutral position Anatomy – Ankle Inversion • Dynamometer Placement: Just medial and proximal to the 1st metatarsal head
Positioning – Ankle INVERSION Subject supine, hips knees and ankle neutral Pull foot towards opposite foot. Placement on inner aspect of foot, just above big toe
Subject supine, heels just off the edge of table and hands on chest • Hips, knees, and ankle in neutral position Anatomy – Ankle Eversion • Dynamometer Placement: Just lateral and proximal to the 5th metatarsal head
Positioning – Ankle INVERSION Subject supine, hips knees and ankle neutral Pull foot away from opposite foot. Placement on outer aspect of foot, just above little toe
Subject standing facing a wall with toes placed 12 inches away from the wall • Must keep hip and knee at 0 degrees (fully extended) throughout testing • Test one leg at a time Anatomy – Ankle PLANTARFLEXION (Heel Raise)
Procedures: Heel Raise Test • Place yardstick behind the calcaneus, and then ask patient to perform a maximal heel raise and hold it. • Record height of the heel raise is on the yardstick with a pencil or piece of tape. • Let patient relax and return to neutral position • Record a second pencil mark or piece of tape is placed on the yardstick exactly 1/2 of the height of the subject’s maximal heel raise. • Place yardstick behind the subject’s heel during testing and the subject must clear the 50% tape height for a given repetition to be counted. • The patient is to perform 1 calf raise every 2 seconds (1 second up and 1 second down). The subject can be “paced” using a watch and vocal cues
Procedures: Heel Raise Test • Subject instructions: • Stand on one leg and perform your maximal number of calf raises staying with the beat of the prompts. • You may lightly touch the wall for balance, but do not lean forward. Keep your knee locked out for all repetitions. • The test continues until patient becomes fatigued and no longer can continue or trunk lean occurs, loss of knee extension, or breaking of required tempo. • Record the number of heel raises above the tape for each leg – only count heel raises above the half-way point