Download
1 / 47
470 likes | 759 Views
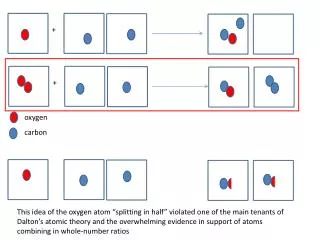
Oxygen. The 10 Most Abundant Elements in the Universe Source: Exploring Chemical Elements and their Compounds; David L. Heiserman, 1992. Composition of the Earth's Atmosphere Source: Definition of the U.S. Standard Atmosphere (1976) CRC Handbook of Chemistry and Physics, 77th Edition. Oxygen.

E N D
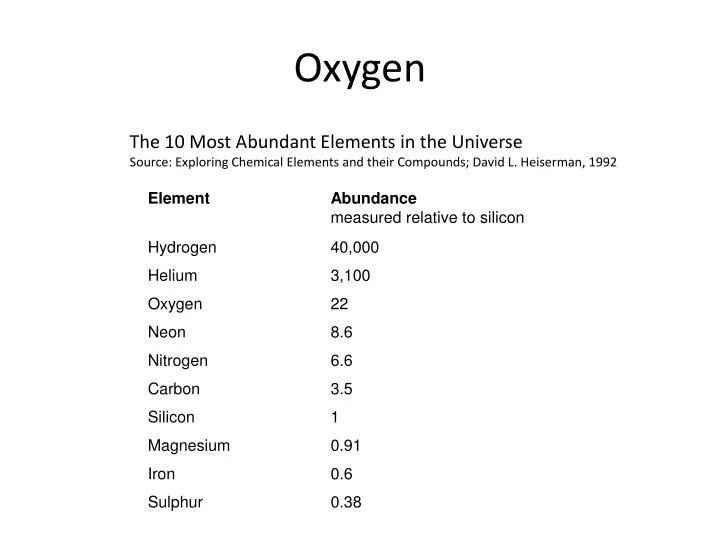
Oxygen The 10 Most Abundant Elements in the Universe Source: Exploring Chemical Elements and their Compounds; David L. Heiserman, 1992
Composition of the Earth's AtmosphereSource: Definition of the U.S. Standard Atmosphere (1976)CRC Handbook of Chemistry and Physics, 77th Edition
Oxygen • Production • Photosynthesis • Where it has all come from • Heating mercuric oxide and nitrates • How it was discovered • Fractional distillation of air • Supply for medicine and industry • Colourless gas, pale blue liquid
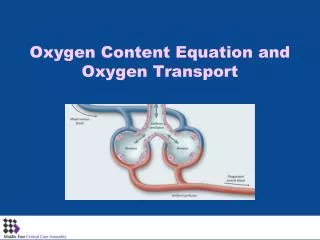
Oxygen Oxygen Cascade Oxygen moves down a stepwise series of partial pressure gradients from the inspired air to the body's cells and their mitochondria.
Oxygen Oxygen cascade interference At 19,000 feet (just above base camp at Mount Everest, the barometric pressure is half that at sea level, and thus, even though the FiO2 is 21%, the PIO2 is only 70mmHg, half that at sea level Increased barometric pressure such as in hyperbaric chambers, the PIO2 will actually be higher More oxygen…but dissolved not on haemoglobin
Oxygen Dr Mark B Smith
Oxygen The amount of oxygen in the bloodstream is determined by; serum haemoglobin level percentage of this haemoglobin saturated with oxygen cardiac output the amount of oxygen dissolved (see below).
EMERGENCY MOBILE MEDICAL UNIT Training Weekend HYPOVENTILATION • A RISE IN PaCO2 CAUSES A FALL IN PaO2 THIS IS THE BASIS OF THE ALVEOLAR GAS EQUATION PaO2 = FiO2(Pb-PaH2O)-PaCO2/0.8
EMERGENCY MOBILE MEDICAL UNIT Training Weekend • TREATMENT • OXYGEN TO OBTAIN SaO2>90% • IF THE PATIENT BECOMES TIRED THE PaCO2 MAY RISE • IF RISING PaCO2 OR DROWSY PROVIDE ASSISTED VENTILATION
EMERGENCY MOBILE MEDICAL UNIT Training Weekend HIGH CONCENTRATIONS OF INSPIRED OXYGEN DO NOT DEPRESS VENTILATION IN PATIENTS WITH ACUTE RESPIRATORY FAILURE
EMERGENCY MOBILE MEDICAL UNIT Training Weekend • OXYGEN THERAPY ON GENERAL WARDS MUST BE PRESCRIBED • TYPE OF OXYGEN DELIVERY SYSTEM • FLOW RATE OF OXYGEN (OR %) • DURATION OF THERAPY • MONITORING TO BE UNDERTAKEN Oxygen is a drug
EMERGENCY MOBILE MEDICAL UNIT Training Weekend OXYGEN DELIVERY SYSTEMS • VARIABLE PERFORMANCE • FIXED PERFORMANCE
VARIABLE PERFORMANCE SYSTEMS NASAL CANNULA • 24-40% DEPENDING ON FLOW RATE • INSPIRED CONCENTRATION VARY BETWEEN BREATHS • DEPENDS UPON RATE AND DEPTH • MAXIMUM FLOW RATE APPROX 4 l/min
VARIABLE PERFORMANCE SYSTEMS SIMPLE FACE MASK • MASK INCREASES RESERVOIR • MINIMAL FLOW RATE APPROX 4 l/min • NO INCREASED INSPIRED OXYGEN ABOVE 15 l/min • INSPIRED OXYGEN OF UP TO 60%
VARIABLE PERFORMANCE SYSTEMS PARTIAL REBREATHING MASKS • FACEMASK AND RESERVOIR BAG • INSPIRED OXYGEN >60% • FLOW RATES OF APPROX 15 l/min REQUIRED
FIXED PERFORMANCE SYSTEMS VENTURI MASK • ENTRAINS AIR • HIGH FLOW MAINTAINS HIGH INSPIRED OXYGEN CONCENTRAION THROUGHOUT RESPIRATORY CYCLE • COLOUR CODED VENTURI HEADS
FIXED PERFORMANCE SYSTEMS ANAESTHETIC MACHINE • Open system • Magill Circuit • Bains system • Maplesons C • Closed system • Circle
EMERGENCY MOBILE MEDICAL UNIT Training Weekend SUMMARY ALL CRITICALLY ILL PATIENTS REQUIRE OXYGEN
British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patient GIFTASUP 2006 Jeremy Powell-Tuck (chair)1, Peter Gosling2, Dileep N Lobo1,3 Simon P Allison1, Gordon L Carlson3,4, Marcus Gore3, Andrew J Lewington5, Rupert M Pearse6, Monty G Mythen6 On behalf of 1BAPEN Medical - a core group of BAPEN, 2the Association for Clinical Biochemistry, 3the Association of Surgeons of Great Britain and Ireland, 4the Society of Academic and Research Surgery, 5the Renal Association and 6the Intensive Care Society. www.bapen.org.uk/pdfs/bapen_pubs/giftasup.pdf
Intravenous fluid • Not one Rx for all • Calculate approximate volume required • Choose the most appropriate IV fluid for task • Dextrose containing solutions should not be used to replace ECF or blood losses • Monitor fluid status
Intravenous fluids • Monitor • Physiological parameters • Cardiovascular • Pulse • Blood pressure • Central venous pressure • Left sided pressures • Pulmonary Artery • Pulmonary Capillary Wedge Pressure • Renal • Urine output • Fluid balance • Blood test • Urea and Electrolytes
Body water compartments. The ability of a solution to expand the plasma volume is dependent on the volume of distribution of the solute, so that while colloids are mainly distributed in the intravascular compartment, dextrose containing solutions are distributed through the total body water and hence have a limited and transient volume expanding capacity. Isotonic sodium-containing crystalloids are distributed throughout the extracellular space and in practice the efficiency of these solutions to expand the plasma volume is only 20-25%, the remainder being sequestered in the interstitial space.
Intravenous fluids Maintenance 1000 N Saline 8 hourly + KCl 20mmol 1000 5% Dextrose 8 hourly + KCl 20mmol 1000 5% Dextrose 8 hourly + KCl 20mmol Or 1000 Dextrose Saline 8 hourly + KCl 20mmol 1000 Dextrose Saline 8 hourly + KCl 20mmol 1000 Dextrose Saline 8 hourly + KCl 20mmol
Intravenous Fluids Resuscitation 500mls N Saline Stat Review 500mls N Saline Stat Review 500mls N Saline Stat Review Colloid Gelofusin Voluven Blood
Composition of some bodily fluids Body Secretion Na+ K+ Cl- HCO3- Volume L/24 hr Saliva 2-85 0-20 16-23 14 0.5-1.5 Gastric Juice 20-60 14 140 0 – 15 2 – 3 Pancreatic Juice 125-138 8 56 85 0.7-2.5 Bile 145 5 105 30 0.6 Jejunal Juice 140 5 135 8 - Ileal Juice 140 5 125 30 - Ileostomy 50 4 25 - 0.5 Colostomy 60 15 40 - 0.1 – 0.2 Diarrhoea 30 – 140 30 – 70 - 20 – 80 Variable Normal Stool 20 – 40 30 - - 0.1-0.25 Sweat 47-60 9 30-40 0-35 0.5 + variable Visible Sweat 58 10 45 - 0.5
Typical properties intravenous fluids Type of Fluid* Sodium Potassium Chloride Osmolarity Weight Plasma volume Mol wt Duration hours Plasma 136-145 3.5-5.0 98-105 280-300 - - 5% Dextrose 0 0 0 278 - - Dextrose 4% saline 0.18% 30 0 30 283 0.9% “normal” saline 154 0 154 308 - 0.2 0.45% “half normal” saline 77 0 77 154 - Ringer’s Lactate 130 4 109 273 - 0.2 Hartmann’s 131 5 111 275 - 0.2 Gelatine 4% 145 0 145 290 30,000 1-2 5% albumin 150 0 150 300 68,000 2-4 20% albumin - - - - 68,000 2-4 HES 6% 130/0.4 154 0 154 308 130,000 4-8 HES 10% 200/0.5 154 0 154 308 200,000 6-12 HES 6% 450/0.6 154 0 154 308 450,000 24-36
Crystalloids • Provide water and electrolytes • Rapidly equilibrate through ECF • Maintenance requirements • Good for replacing ECF depletion • Intravascular expansion short lived • Cheap • Hypoallergenic • Long shelf life
Colloids • Contain larger molecules that remain in the plasma longer • Gelatins • Starches • Exert oncotic pressure • Less volume required to generate intravascular expansion • Allergic reactions • Expensive • Shorter shelf life
Intravenous fluid Summary Fluids have specific roles Maintenance Replacement of losses Monitor
After ABC Mark B Smith
After ABC • What can go wrong • Respiration • Cardiovascular • Neurological
After ABC • Symptoms • Pain • Confusion • Shortness/difficulty breathing • Signs • Tachycardia/hypotension/capillary refill • AVPU/GCS • Respiratory rate • Oxygen saturation
After ABC • Looking for • Respiratory • Pneumothorax/Haemothorax • Aspiration/obstruction • Cardiovascular • Haemorrhage • Cardiac failure
After ABC • Neurological • Loss of consciousness • Pupils • Space occupying lesion • Blood sugar • Hyperglycemia and hypoglycemia should be avoided • Keep the blood glucose value in the range of 80 to 110 mg/dl (4-8mmols/l) • Is the patient a diabetic? Sugar tablets/drinks v insulin • 5% population are diabetic
After ABC • Pneumothorax • Trachea deviation • Hyper-resonant • Haemothorax • Tracheal deviation • Hypo-resonant/dull
Chest drain • Chest drain insertion • http://www.youtube.com/watch?v=B0wGmWn8Ubs • http://www.youtube.com/watch?v=hQlt57AyQmg • Needle aspiration • http://www.youtube.com/watch?v=UvHJ4pjNh2Q&feature=related
Intravenous access • Difficult • Cold • Vaso-constricted • Access Leads to FAILURE!! And cross medical staff!!!!
Intra osseous cannulation • Demonstration1 Rep and lady • http://www.youtube.com/watch?v=VrQppt6sMiM • http://www.youtube.com/watch?v=sirU0Q1TEcU&feature=related • Demonstration 2 Pain • http://www.youtube.com/watch?feature=endscreen&v=ff_vqePp_jw&NR=1 • Demonstration 3 Leg • http://www.youtube.com/watch?v=NPwmoRScJ-U&feature=related • Demonstration 4 Company/long • http://www.youtube.com/watch?v=jBtm3MUv-B0&feature=related • Demonstration 5 Mistakes • http://www.youtube.com/watch?v=YXfyL8kvFTg&feature=related
http://www.youtube.com/watch?v=nt56jMvA71c&feature=related • http://www.youtube.com/watch?v=qYQn4TSjge4&feature=related • http://www.youtube.com/watch?feature=endscreen&v=3ZDpiZHbrW4&NR=1
After ABC Thank you Any questions