Download
1 / 43
440 likes | 650 Views
Explore the ABO blood group system, its importance in transfusion compatibility, and the significance of antibody screening. Learn about other key blood group systems and compatibility testing procedures.

E N D
Although there are over 300 known red blood cell antigens organized into 35 blood group systems, routine blood typing is usually concerned with only two systems: the ABO and Rh blood group systems. Antibody screening helps to identify antibodies against several other groups of red blood cell antigens. • Some of the other groups are the Duffy, Kell, Kidd, MNS, and P systems
ABO • ABO • 001 • 4 • MNSs • MNS • 002 • 37 • P • P1 • 003 • 1 • Rh • RH • 004 • 47 • Lutheran • LU • 005 • 18 • Kell • KEL • 006 • 21 • Lewis • LE • 007 • 3 • Duffy • FY • 008 • 6 • Kidd • JK • 009 • 3 • Diego • DI • 010 • 2 • Cartwright • YT • 011 • 2 • BLOOD GROUP SYSTEMS • CONVENTIONAL NAME • ISBT SYMBOL • ISBT NUMBER • ANTIGENS • * • *
CONVENTIONAL NAME • ISBT SYMBOL • ISBT NUMBER • ANTIGENS • Xg • XG0 • 012 • 1 • Scianna • SC • 013 • 3 • Dombrock • DO • 014 • 5 • Colton • CO • 015 • 3 • Landsteiner-Wiener • LW • 016 • 3 • Chido/Rogers • CH/RG • 017 • 9 • Hh • H • 018 • 1 • Kx • XK • 019 • 1 • Gerbich • GE • 020 • 7 • Cromer • CROMER • 021 • 10 • Knops • KN • 022 • 5 • Indian • IN • 023 • 2 • Ok • OK • 024 • - - • Raph • RAPH • 025 • - - • JMH • JMH • 026 • - - • BLOOD GROUP SYSTEMS
ABO blood group antigens present on red blood cells and IgM antibodies present in the serum
Why do we have Anti-A or Anti-B Antibodies??? • Viruses transmitted from the respiratory tracts of humans to other humans drag along various antigens including ABO blood group antigens. • Prime the newborn’s immune system. • Reduces transmissibility of viruses within a population.
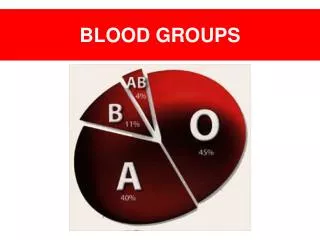
Population Distribution of • Major Blood Groups • O Rh pos 38% • O Rh neg 7% • A Rh pos 34% • A Rh neg 6% • B Rh pos 9% • B Rh neg 2% • AB Rh pos 3% • AB Rh neg 1%
Recipient • Donor • O- • O+ • A- • A+ • B- • B+ • AB- • AB+ • O- • O+ • A- • A+ • B- • B+ • AB- • AB+ • Red blood cell compatibility table
Plasma compatibility table • Recipient • Donor • O • A • B • AB • AB • A • B • O
Other Blood Groups • No naturally occurring antibodies • Immune response requires • previous exposure • Weaker titers of univalent antibodies
Why do we care? • Compatibility testing is done to avoid • a hemolytic transfusion reaction • If the Host or Recipient recognizes • the donor RBC surface antigens as foreign, • the host will mount an immune response • to the donor RBC’s
Major Blood Groups • Rhesus • 50 Antigens make up the • Rhesus Blood Group • The most significant is the • D antigen
There is no naturally occurring • Anti D Antibodies • Production of Anti D in the • RH negative recipient • requires previous exposure • to the D antigen • (in utero or by transfusion)
If red cells are administered • to an ABO- or D-incompatible recipient, • the recipient will mount an • antibody response to the foreign • RBC surface antigens • IgM is polyvalent • and fixes complement
Donor RBC’s coated with host antibodies • Stiffer RBC membrane • Susceptible to attack by • splenic macrophages
What is compatibility testing? • Also called pretransfusion testing • Purpose: • To select blood components that will not cause harm to the recipient and will have acceptable survival when transfused • If properly performed, compatibility tests will confirm ABO compatibility between the component and the recipient and will detect the most clinically significant unexpected antibodies
COMPATIBILITY TESTING • Processing the specimen: • ABO Group determined (forward and reverse) • D typing determined • Antibody screen will be performed • ABO/Rh identical or compatible blood will be made available
Sample Identification • The sample should also have the full patient name, hospital number, and physician • Date and time of collection, phlebotomist’s initials • All of this should be on the request form and the sample
Serological Testing • 3 tests: • ABO/Rh • Antibody detection/identification • Crossmatch
ABO/Rh Typing • In the ABO typing, the forward and reverse MUST match • In the Rh typing, the control must be negative • Both of these will indicate what type of blood should be given
Typing of ABO Blood Group Forward Reaction: The patient’s (recipient’s) red blood cells are mixed with monoclonal antibodies to either A or B antigens to see if they clump. Reverse Reaction: Commercially available A or B cells are mixed with the patient’s (recipient’s) plasma in two separate tubes.
ABO TYPING • Front or forward type using monoclonal anti-A and anti-B (commercial) • The sample is diluted to Hct 0.08, the commercial antibodies added & the test tube is centrifuged • The RBC’s are then examined for clumping (gross observation, gel suspension)
Anti A • Anti B • Anti A • Anti B • A • B • Anti A • Anti B • Anti A • Anti B • AB • O
A • A • A • A • B • B • B • B ABO TYPING Back or reverse type with A and B cells • Commercially available A and B cells are added to two tubes of plasma • AB B A O
How do we know whether or not the host (or recipient) has antibodies to minor blood group antigens? • Add commercial RBC’s with known important minor antigens on their surface to host (or recipient) plasma and centrifuge. Then incubate at body temperature for 15-30 minutes • Then add rabbit antiglobulin
Antibody screen • Also called the indirect Coombs test or the indirect antiglobulin test • The antibody screen will detect the presence of any unexpected antibodies in patient serum • If antibodies are detected, identification should be performed using panel cells (with an autocontrol) • IS • 37° (LISS) • AHG
Screening • The patient’s serum is mixed with a set of commercial red cells with known minor antigens on the surface and tested to see if the patient has any antibodies that reacted with these minor antigens
If recipient antibodies have coated • commercial RBC surfaces
Rabbit antiglobulin will bind to the • Antibodies and the RBC’s will clump
ANTIBODY SCREENING • Detection of unexpected clinically significant antibodies against the minor blood group system antigens • Positive in between 0 - 8% of samples depending on the population
Crossmatching • Purpose: • Prevent transfusion reactions • Increase in vivo survival of red cells • Double checks for ABO errors • Another method of detecting antibodies
Crossmatching • The patient’s (recipient’s) serum is mixed with the donor red cells being transfused to test for agglutination.
Crossmatches • According to the AABB Standards: The crossmatch “shall use methods that demonstrate ABO incompatibility and clinically significant antibodies to red cell antigens and shall include an antiglobulin phase”
Crossmatch No agglutination ~ compatible Agglutination ~ incompatible Donor RBCs (washed) Patient serum
Crossmatches… Will Verify donor cell ABO compatibility Detect most antibodies against donor cells Will Not Guarantee normal survival of RBCs Prevent patient from developing an antibody Detect all antibodies Prevent delayed transfusion reactions
Summary • The crossmatch “shall use methods that demonstrate ABO incompatibility and clinically significant antibodies to red cell antigens • If an emergency transfusion is required after type and screen alone, an immediate-phase crossmatch is performed before transfusion (an abbreviated format ) • If crossmatched blood is not ready to give, use type-specific or type O Rh-negative cells