Download
1 / 19
190 likes | 378 Views
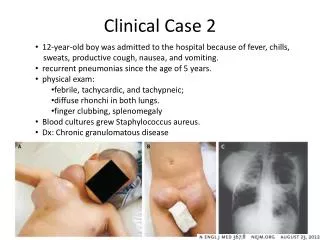
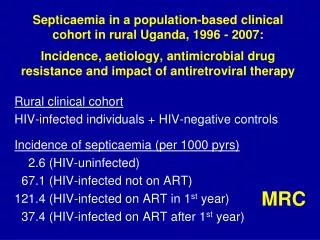
ANRS C05 HIV-2 Cohort Clinical case management . S Matheron Hopital Bichat – Claude Bernard Université Denis Diderot Paris 7. Open, multi-centric national cohort - since 1994 - 121 investigating centers - 847 patients included (June, 2011) - + 155 since 2007. Year of HIV-2 diagnosis.

E N D
ANRS C05 HIV-2 CohortClinical case management S Matheron Hopital Bichat – Claude Bernard Université Denis Diderot Paris 7
Open, multi-centric national cohort - since 1994 - 121 investigating centers - 847 patients included (June, 2011) - + 155 since 2007 Year of HIV-2 diagnosis ANRS HIV-2 cohort • Inclusion criteria • HIV-2 Infection only • ≥ 18 years old, • > 1 year in France • 60% women • 50% > 40 years • 75% fromsubsaharanAfrica • (WA) • 24% previouslygivencART • Clinical, epidemiological, biological and therapeutic follow-up • / 6 months* • Virological follow-up • untreated patients • / 6 months * • / 3 months if plasma VL>100copies/ml • treated patients • M1, / 3 months • * + in case of intermediate event IAS 2011, ANRS satellite, HIV-2, 19th July
ANRS CO5: Patients’ characteristics C (Tuberculosis 44 %) B A • At inclusion • CDC stage (n=719) • A • B • C N 600 31 88 87 345 132 264 (%) 83.3% 4.4% 12.3% 37% 47% 18% 35% 516 302 138 CD4 counts (median) 18% 30% 51% 27% 26% 95% 70% IAS 2011, ANRS satellite, HIV-2, 19th July
ANRS CO5: Patients’ characteristics • At inclusion • CDC stage (n=719) • A • B • C • Plasma RNA >100 copies/ml (n=235) • CD4+ T lymphocytes • >500/mm3 • [300-500]/mm3 • <300/mm3 • Follow-up (n=702) • Lost of follow-up • cART initiation (n=488) • Survival at 5 years • Non progression to AIDS at 5 years N 600 31 88 87 345 132 264 (%) 83.3% 4.4% 12.3% 37% 47% 18% 35% 516 302 138 CD4 counts (median) Median : 2.8 log 18% 30% 51% Detectable plasma RNA 27% 26% 95% 70% IAS 2011, ANRS satellite, HIV-2, 19th July
ANRS CO5: Patients’ characteristics • At inclusion • CDC stage (n=719) • A • B • C • Plasma RNA >100 copies/ml (n=235) • CD4+ T lymphocytes • >500/mm3 • [300-500]/mm3 • <300/mm3 • Follow-up (n=702) • Lost of follow-up • cART initiation (n=488) • Survival at 5 years • Non progression to AIDS at 5 years N 600 31 88 87 345 132 264 (%) 84% 4% 12% 38% 47% 18% 35% 516 302 138 CD4 counts (median) Median : 2.8 log 18% 30% 51% Detectable plasma RNA 27% 26% 95% 90%
ANRS CO5: Patients’ characteristics • At inclusion • CDC stage (n=719) • A • B • C • Plasma RNA >100 copies/ml (n=235) • CD4+ T lymphocytes • >500/mm3 • [300-500]/mm3 • <300/mm3 • Follow-up (n=702) • Lost of follow-up • cART initiation (n=488) • Survival at 5 years • Non progression to AIDS at 5 years N 600 31 88 87 345 132 264 (%) 84% 4% 12% 38% 47% 18% 35% 516 302 138 CD4 counts (median) Median : 2.8 log 18% 30% 51% Detectable plasma RNA 27% 26% 95% 90% • Natural history • Response to cART
Comparison of viro-immunological marker changes between HIV-1 and HIV-2-infected patients (n= 6707/ 592) Drylewicz J et al, AIDS, 2008 _9 cells/ml PY _0.04%/year HIV-2 HIV-1 _49 cells/ml PY _1.01%/year IAS 2011, ANRS satellite, HIV-2, 19th July
Comparison of viro-immunological marker changes between HIV-1 and HIV-2-infected patients Drylewicz J et al, AIDS, 2008 HIV-2 _11 cells/ml PY _49 cells/ml PY HIV-1 IAS 2011, ANRS satellite, HIV-2, 19th July
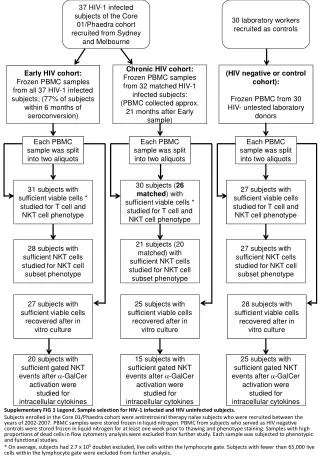
ANRS CO5 HIV-2 HIV-2 patients with at least one follow-up available since 2009 with known date of HIV diagnosis n=357 HIV-2 infection ≥ 8 years n=221 Non progressor and HIV controllers patients At least 3 plasma viral loads and CD4 in the last five years n=176 Asymptomatic patients n=119 Antiretroviral naïve patients n=60 CD4 nadir ≥ 500 cells/µl n=36 « LTNP* » HIV infection ≥ 10 years n=44 6% CD4 nadir ≥ 600 cells/µl n=26 « LTNP** » 90% of pVL ≤ 500 copies/ml n=40 « HIV controlers » 9% CD4 slope ≥ 0 over the last 5 years n=8 « Elite-LTNP » 1,5% Among which 5 HIV controlers and 5 Elite controlers Last pVL ≤ 100 copies/ml n=37 « Elite-controlers » 8;8% Among which 23 LTNP and 5 Elite LTNP
Treatment • Clinical case management in the setting of cohortstudy • features and specificities of HIV-2 infection • Fewer patients • Slower infection • Fewer clinical events • Slower CD4 decrease • Lower viral replication • Viral load quantification • Threshold 100 cp/ml • Fewer potent drugs • Resistance pathway • data throughretrospectivestudies • currentlyhigherevidence-basedlevel of knowledge on treatment • Viral load can’t be used as primary endpoint • Limited options for second and further lines
ANRS CO5: Response to cART • lopinavir/r - containingcART(29 naïve patients, 2002-2007) • Responseat W24 : + ≥ 50 CD4 at M6, and VL < 100 cp/ml = 59% • Median CD4 gain • W24 +71 (28) • W48 +122 (19) • W96 +132 (13) • Estimated CD4 slope • W0-W12 : +23 CD4/mm3/mth • W13-W96: +8 CD4/mm3/mth • A Benard , AIDS, 2008 IAS 2011, ANRS satellite, HIV-2, 19th July
Comparison of viro-immunological marker changes between HIV-1 and HIV-2-infected patients Drylewicz, AIDS, 2008 + 46/y +59/mth match according to VL at D0 (>3.5 versus 3.5 log10 cp/ml) +24/mth - 2,88/y - 1.56 log/m - 0,62 log/m IAS 2011, ANRS satellite, HIV-2, 19th July
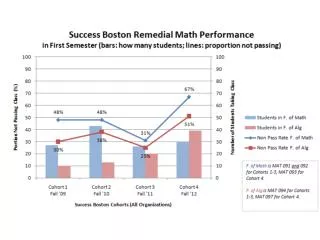
ACHIeV2e : 3 INTI vs 2 INTI+PI/r as 1st line M4-M12 +76/mm3/year - 60/mm3/year p=0.002 M0-M3 +12/mm3/month + 6/mm3/month p=0.24 N=44 N=126 Estimated CD4 cell count changes (n=158) Bénard, CID, 2011 IAS 2011, ANRS satellite, HIV-2, 19th July
ACHIeV2e : 3 INTI vs 2 INTI+PI/r as 1st line M0-M3 -0.2 log10 cp/month -0.4 log10 cp/month p=0.02 M4-M12 +1.2 log10 cp/ml/year -0.12 log10 cp/ml/year p=0.19 Estimated HIV-2 RNA changes in patients with detectable values at treatment initiation (n=67) Bénard, CID, 2011 IAS 2011, ANRS satellite, HIV-2, 19th July
ANRS CO5 raltegravirincludingcART • Case reports • Experienced patients (several cART failures)
Clinical case management Recommendations • First line • 2 INTI + PI/r : LPV, or DRV/r or SQV/r • 2nd line ? • Samestrategy as for HIV-1 • Tolerance, observance, PK, and genotype • Integraseinhibitors • Anti CCR5
Clinical case management Questions : • Start earlier ? • Start stronger ? • impact on tolerance, observance ? • which options for 2nd line ? • Clinicalresearch • Evaluation of new treatmentstrategies • International network • Randomized trial
Laboratories Belgium: Patrick GOUBAU *, Jean RUELLE Canada: Marc WAINBERG France: BrigitteAUTRAN Françoise BRUN-VEZINET * Florence DAMOND*, Diane DESCAMPS * François SIMON * Gambia: AkumAVEIKA, MatthewCOTTEN Sarah ROWLAND-JONES Germany: BerndKUPFER Italy: ClaudiaBALOTTA * CarloTORTI Netherlands: Martin SCHUTTEN Portugal: Vitor DUQUE, Joao VAZ RicardoCAMACHO *, Perpetua GOMES * Sweden: JanALBERT USA: GeoffreyGOTTLIEB UK: Deenan PILLAY, Bridget FERNS, Jeremy GARSON HIV-2 cohort Clinical centres Germany: Jürgen ROCKSTROH, Carolynne SCHWARZE-ZANDER Netherlands: Frank DE WOLF *, Ard van SIGHEM *, PeterREISS Maarten SCHIM VAN DER LOEFF Portugal: Francisco ANTUNES* Emilia VALADAS * Kamal MANSINHO * Spain: Vicente SORIANO* Ana TREVINO * Carlos TORO * Berta RODES * Switzerland: Jürg BÖNI * Martin RICKENBACH * Alexandra CALMY * UK: JaneANDERSON JenniferTOSSWILL Investigateur coordonnateur Sophie Matheron SMIT, Bichat-Claude Bernard Coordination virologique Francoise Brun-Vézinet , Laboratoire de Virologie, Bichat-Claude Bernard Florence Damond Coordination immunologique Brigitte Autran, Laboratoire d’immunologie cellulaire, Pitié-Salpétrière Coordination méthodologique Genevieve Chêne , NSERM U593, Bordeaux Antoine Bénard • Monitorage • Dien Le, SMIT, Bichatt • Statistique et informatique • Audrey Taïeb, INSERM U593
ANRS CO5 HIV-2 cohort • Acknowledgments • Patients • Investigators 19