Download
1 / 113
1.13k likes | 1.15k Views
Explore the intricate mechanisms of hemodynamic disorders including thromboembolic disease, shock, edema, hyperemia, congestion, hemorrhage, and more. Uncover the underlying causes and manifestations of these conditions.

E N D
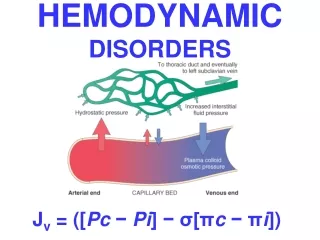
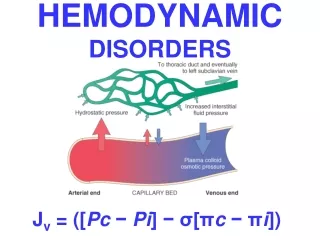
HEMODYNAMIC DISORDERS Jv = ([Pc − Pi] − σ[πc − πi])
Hemodynamic Disorders • Thromboembolic Disease • Shock
Overview • Edema (increased fluid in the ECF) • Hyperemia (INCREASED flow) • Congestion (INCREASED backup) • Hemorrhage (extravasation) • Hemo-stasis* (opposite of thrombosis) • Thrombosis (clotting blood) • Embolism (downstream travel of a clot) • Infarction (death of tissues w/o blood) • Shock (circulatory failure/collapse)
EDEMA= ↑ECF • ONLY 4 POSSIBILITIES!!! • Increased Hydrostatic Pressure • Reduced Oncotic Pressure • Lymphatic Obstruction • Sodium/Water Retention
WATER • 60% of body • 2/3 of body water is INTRA-cellular • The rest is INTERSTITIAL • Only 5% is INTRA-vascular • EDEMA is SHIFT to the INTERSTITIAL SPACE FROM EITHER DIRECTION • HYDRO- • -THORAX, -PERICARDIUM, -PERITONEAL • EFFUSIONS, ASCITES, ANASARCA
INCREASED HYDROSTATIC PRESSURE (i.e.,VENOUS) • Impaired venous return • Congestive heart failure • Constrictive pericarditis • Ascites (liver cirrhosis) • Venous obstruction or compression • Thrombosis • External pressure (e.g., mass) • Lower extremity inactivity with prolonged dependency • Arteriolar dilation • Heat • Neurohumoral dysregulation
REDUCED PLASMA ONCOTICPRESSURE (HYPOPROTEINEMIA) • Protein-losing glomerulopathies (nephrotic syndrome) • Liver cirrhosis (ascites) • Malnutrition • Protein-losing gastroenteropathy
LYMPHATIC OBSTRUCTION(LYMPHEDEMA) • Inflammatory • Neoplastic • Postsurgical • Postirradiation
Na+ RETENTION • Excessive salt intake with renal insufficiency • Increased tubular reabsorption of sodium • Renal hypoperfusion Increased renin-angiotensin-aldosterone secretion
INFLAMMATION • Acute inflammation (r,c,d,T) • Chronic inflammation • Angiogenesis
CHF EDEMA-2 REASONS • INCREASED VENOUS PRESSURE DUE TO FAILURE • DECREASED RENAL PERFUSION, triggering of RENIN-ANGIOTENSION-ALDOSTERONE complex, resulting ultimately in SODIUM RETENTION
HEPATIC ASCITES- 2 REASONS • PORTAL HYPERTENSION • HYPOALBUMINEMIA
RENAL EDEMA- 2 REASONS • SODIUM RETENTION • PROTEIN LOSING GLOMERULOPATHIES (NEPHROTIC SYNDROME)
EDEMA • SUBCUTANEOUS (“PITTING”) • “DEPENDENT” • ANASARCA • LEFT vs RIGHT HEART • PERIORBITAL • PULMONARY • CEREBRAL (closed cavity, no expansion) • HERNIATION of cerebellar tonsils • HERNIATION of hippocampal uncus over tentorium • HERNIATION, subfalcine
Transudate vs. Exudate • Transudate (water) • results from disturbance of Starling forces • specific gravity < 1.012 • protein content < 3 g/dl, LDH LOW, ↓ Cells • Exudate (goo) • results from damage to the capillary wall • specific gravity > 1.012 • protein content > 3 g/dl, LDH HIGH, ↑ Cells
HYPEREMIA Active Process CONGESTION Passive Process Acute or Chronic
CONGESTION • LUNG, best example R. CHF • ACUTE • CHRONIC, hemosiderin • LIVER, best example L. CHF • ACUTE • CHRONIC, necrosis • CEREBRAL
ACUTE PASSIVE HYPEREMIA/CONGESTION, LUNG septae alveoli
Kerley B Air Bronch-ogram
HEMORRHAGE • EXTRAVASATION beyond vessel • “HEMORRHAGIC DIATHESIS” • HEMATOMA (implies MASS effect) • “DISSECTION” • PETECHIAE (1-2mm) (PLATELETS) • PURPURA <1cm • ECCHYMOSES >1cm (BRUISE) • HEMO-: -thorax, -pericardium, -peritoneum, HEMARTHROSIS • ACUTE, CHRONIC
EVOLUTION of HEMORRHAGE • ACUTE CHRONIC • PURPLE GREEN BROWN • HGB BILIRUBIN HEMOSIDERIN
HEMO”STASIS” • OPPOSITE of THROMBOSIS • PRESERVE LIQUIDITY OF BLOOD • “PLUG” sites of vascular injury • THREE COMPONENTS • 1 VASCULAR WALL, i.e., endoth/ECM • 2 PLATELETS, “PRIMARY” COAG. • 3 COAGULATION CASCADE, or “SECONDARY” COAGULATION
SEQUENCE of EVENTSfollowing VASCULAR INJURY • ARTERIOLAR VASOCONSTRICTION • Reflex Neurogenic • Endothelin, from endothelial cells • THROMBOGENIC ECM at injury site • Adhere and activate platelets • Platelet aggregation (1˚ HEMOSTASIS) • TISSUE FACTOR released by endothelium, plats. • Activates coagulation cascadethrombinfibrin (2˚ HEMOSTASIS) • FIBRIN polymerizes, TPA limits plug
PLAYERS • 1) ENDOTHELIUM • 2) PLATELETS • 3) COAGULATION “CASCADE”, or SEQ.
ENDOTHELIUM • NORMALLY • ANTIPLATELET PROPERTIES • ANTICOAGULANT PROPERTIES • FIBRINOLYTIC PROPERTIES • IN INJURY • PRO-COAGULANT PROPERTIES
ENDOTHELIUM-JEKYLL • ANTI-Platelet PROPERTIES • Protection from the subendothelial ECM • Degrades ADP (inhib. Aggregation) • ANTI-Coagulant PROPERTIES • Membrane HEPARIN-like molecules • Makes THROMBOMODULIN Protein-C • TISSUE FACTOR PATHWAY INHIBITOR • FIBRINOLYTIC PROPERTIES (TPA)
ENDOTHELIUM-HYDE • PROTHROMBOTIC PROPERTIES • Makes vWF, which binds PlatsColl • Makes TISSUE FACTOR (with plats) • Makes Plasminogen inhibitors
ENDOTHELIUM • ACTIVATED by INFECTIOUSAGENTS • ACTIVATED by HEMODYNAMICS • ACTIVATED by PLASMA • ACTIVATED by ANYTHING which disrupts it, including physical trauma “DISRUPTION”
PLATELETS • ALPHA GRANULES • Fibrinogen • Fibronectin, a big CAM • Factor-V, Factor-VIII • Platelet factor 4, TGF-beta • DELTA GRANULES (DENSE BODIES) • ADP/ATP, Ca+, Histamine, Serotonin, Epineph. • With endothelium, form TISSUE FACTOR
NORMAL platelet on LEFT, “DEGRANULATING” ALPHA GRANULE ON RIGHT AT OPEN WHITE ARROW