Download
1 / 69
690 likes | 1.08k Views
PATHOPHYSIOLOGY OF ENDOCRINE SYSTEM DM.Prof.Yu.I.Bondarenko. Role of endocrine system in vital activity of the organism.

E N D
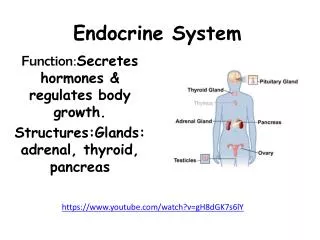
Role of endocrine system in vital activity of the organism • The endocrine system is the most important regulatory system. It carries out regulatory influence by means of hormones practically on all functions of an organism – metabolism , growth, reproduction, mental activity, adaptation, functional activity of all organs. • Hormones can be synthesized: а) by epithelial cells (one’s own glandular ephithelium ); b) by neuroendocrine cells (hypothalamic cells); c) by myoendocrine cells (muscular fibres of heart atriums).
Role of endocrine system in vital activity of the organism • According to chemical nature they differentiate: а) steroid hormones (mineral – and glucocorticoids, female and male sexual hormones); b) derivatives of aminoacids (thyreoid hormones, catecholamines, melatonine); c) protein and peptide hormones (releasing-hormones, vasopressin, oxytocin, hormones of adenohypophysis, insuline, glucagone, parathyrin, calcitonine). • According to functional effects hormones can be: а) affectors (act directly on organs - targets); b) tropic (regulate synthesis of effecting homones); c) releasing-hormones (regulate synthesis and secretion of tropic hormones).
Etiology of endocrinedisorders Reasonsofdisorders: mental trauma, necrosis, tumor, inflamatory process, bacterial and viral infections, intoxications, local disorders of blood circulation (hemorrhage, thrombosis), alimentary disorders (deficiency of iodine and cobalt in food and drinking water, redundant consumption of carbohydrates), ionising radiation, inherent chromosome and gene defects.
Types of endocrine disorders • 1. Hyperfunction of endocrine glands • 2. Hypofunction of endocrine glands • 3. Disfunction of endocrine glands Disfunction is characterized by different changes of hormonal production and production physiologic active precursors of their biosynthesis in the same endocrine gland or synthesis and entrance in blood of atypical hormonal products.
Pathogenesis of endocrine disorders • 1. Disorders of endocrine glands regulation – disregulatory disorders; • 2.Disordersof hormones biosynthesisand their secretion – glandular disorders; • 3.Disorders of the transport, reception and metabolism of hormones – peripheral disorders.
Disorders of endocrine gland regulation • 1. Nervous (impulse-mediators) or parahypophysis regulation.By means of direct nervous influences the activity of following structures is regulated: а) adrenal medulla; b) neuroendocrine structures of hypothalamus; c) epiphysis. • 2. Neuroendocrine or transhypophysar regulation. It is carried out by neuroendocrine cells of hypothalamus, which transform nervous impulses in specific endocrine process.Releasing-hormones are synthesized, which regulate activity of adenohypophysis.
Disorders of endocrine gland regulation • 3. Endocrine regulation.One hormones influence on synthesis and secretion of the others. An example of this mechanism is the influence of adenohypophysis tropic hormons on activity of adrenal cortex, thyroid gland, sexual glands. • 4. Non-endocrine humoral regulationis carried out by unspecific humoral factors, in particular by metabolites, ions.
Disorders of endocrine gland regulation • Pathological processes whichprimaryare developed in hypothalamus lead to disorders of transhypophysar and parahypophysar regulation of endocrine glands function. • The activity of hypothalamic centres can be disturbed alsosecondary in connection with disorders in limbic system (hypocampus, tonsil, olfactory brain) and upper parts of central nervous system which are closely connected with hypothalamus. • The large role belongs to mental trauma and other stress influences.
Disorders of endocrine gland regulation Transhypophysar regulationincludes synthesis of peptides, which are moving in axons and reach adenohypophysis in neurosecretory cells of mediobasal part of hypothalamus. Here they either stimulate or inhibit formation of tropic hormones. Stimulating peptides are called liberinesor releasing-factors: thyroliberin, gonadoliberin, somatoliberin etc. Inhibiting peptides are named statines– thyrostatin, somatostatin etc. Their ratio among themselves is determined formation of appropriate tropic hormone. Formation of tropic hormones begins in adenohypophysis – somatotropic (STH), gonadotropic (GTH) etc. Tropic hormones act on appropriate targets and stimulate derivation of hormones in appropriate glands, and STH stimulates formationof somatomedines in tissues – polipeptide hormones.
Disorders of endocrine gland regulation By means of parahypophysar mechanismsecretion, vessel and trophic influence of CNS on the function of endocrine glands is carried out . For adrenal medulla, Langerhans’ islets and parathyroid glands it is a major pathway of their regulation. In realization of the function of other glands both pathways of regulation take place. So, the function of thyroid gland is determined not only by TTH, but also by sympathetic impulsation. The direct irritation of sympathetic nerves increases absorption of iodine by the gland, synthesis of thyroid hormones and their secretion. Denervation of ovaries causes their atrophy and weakens response on gonadotropic hormones. The disorders of trans- and parahypophysar regulation leads to disfunction of endocrine glands. The disturbanc of one gland function is called monoglandularprocess, several glands – pluriglandular process. The disorders of the glandular function can be partial, when production of only one hormone is disturbed, or total, when secretion of all hormones is changed.
Role of mechanisms feedback bond in endocrine disturbances The mechanism of feedback bond is obligated link in self regulation of glandular activity. The essence of negative adverse effects is that formed hormones oppress activity of structures which carry out the previous stages of regulation. Thereforethe increase of secretion of effectory hormone through certain parts causes decrease of its formation and entering in blood, and on the contrary, the decreasing of the hormone contents in blood causes increase of intensity of its formation and secretion. In this way regulation of cortizol secretion, thyroid and sexual hromones is carried out. By the principle of the mechanism of feedback bond inhibition of the function (even atrophy) of the gland during treatment by their or other hormones can occur.
Disorders of hormones biosynthesis and their secretion • 1. Changesof amount of functionally active endocrine cells a) decrease of their amount (removal of gland or its part, damage, necrosis), that results to endocrine hypofunction; b)increase of their amount (benignt and malignant tumors of glandular epithelium) that is accompanied by features of endocrine hyperfunction. • 2. Qualitative changes in cells: a) disorders of biosynthesis of hormones; b) disorders of processes of their secretion. • The main reasons of protein-peptide hormones synthesis disorders are: 1) disorders of transcription; 2) disorders of translation; 3) deficiency of essential aminoacids; 4) deficiency of ATP; 5) disorders of posttranslatory modification and activation.
Disorders of transport, reception and hormones metabolism 1. Disorders of the hormones transport in organism. 2. Disorder of metabolic inactivation of hormones. 3. Disorders of interaction of hormones with peripheral cells - targets. All hormones associated with proteins in blood and circulate in two forms – connected and free. Connected hormone is biologically inactive. Free form of hormone is active. The disorders of the hormone transport in an organism can appear in two types of endocrine function disorders: а) hypofunction – increase of hormone binding and decrease of its contents in the free form; b) hyperfunction – decrease of hormone binding and increase in blood of concentration of the free form.
Disorders of endocrine functions, connected with disturbances of interaction of hormones with peripheral cells The influence of hormones on cells - targets is carried out througtheir action on specific proteins – receptors and is performed in three ways: 1) influences on permeability of biological membranes; 2) stimulation or inhibition of enzymes activity; 3) influences on the genetic apparatus of a cell. Types of hormones cytoreception. • 1. Membrane type of cytoreception. It is the main mechanism of action of protein- peptide hormones and catecholamines. Nowadays we known secondary messengers which are represented by the following substances: a) cyclic nucleotides - cAMP, cGМP; b) ions of Са++; c) phospholipide messengers- diacilglycerol (DAG) and inozitoltriphosphate (ITP). The specificity of the answer of a cell on this or other hormone is determined by specificity of the receptor, which is connected only with a certain hormone, and also by nature of specific to a cell proteinkinase and protein substrats.
Disorders of endocrine functions, connected with disturbances of interaction of hormones with peripheral cells • 2. Intracellular type of cytoreception. It is in the base of mechanism of steroid and thyroid hormones action. The blockade of hormonal receptor is the widespread mechanism, which results to hormonal insufficiency: active hormone does not find receptor on a cell or in it because of receptor loss or fixing on its surface of antagonist, conformation changes of the receptor, which interfere connection with the hormone. Usually concentration of hormone in such cases is normal or increased. The introduction of the hormones with the medical purpose is not accompanied by appropriate effect.
Disorder of endocrine functions, connected with disturbances of hormones metabolis The destruction of protein-peptide hormones is realized in liver by means of peptidase enzymes. The disturbances of hormone metabolism transformations can stimulate development of peripheral disorders of endocrine function. So, in case of decrease of hormones inactivation their contents in blood is increased, that appears in glands hyperfunction. And on the contrary, the accelerated transformation of hormones in their inactive forms is accompanied by development of endocrine hypofunction. In hepatitis and liver cirrhosis hormone metabolism is oppressed.
Disturbances of hypophysis functions.Hypofunction of adenohypophysis (hypopituitaritism) There are panhypopituitarity and partial hypopituitarity. Panhypopituitarity – is decrease of formation of all adenohypophysis hormones. Clinical forms of panhypopituitarity: 1. Hypophysar Simond’s cachexia ; 2.Postpartal necrosis of hypophysis – syndrome of Schegan; 3.Chromophobe hypophysis adenomas, i.e. tumors, which grow from chromophobe cells. Clinical manifestations of panhypopituitarity are connected with deficiency of adenohypophysis hormones and disorders of peripheral endocrine glands activity(thyroid gland, cortex of adrenal, sexual glands).
Hypophyseal Simond’s cachexia
Disturbances of functions of hypophysis.Hypofunction of adenohypophysis (hypopituitaritism) The first symptoms of lesion of adenohypophysis occur in damageof70-75 %glandular tissue, and for development of complete picture of panhypopituitarity necessary destruction of 90-95%adenohypophysis. Vascular disorders in hypophysis and hypothalamus (most frequently postpartal longtime spasm of brain vessels and hypophysis owing to hemorrhage), trauma of the skull basis, tumor of hypophysis and hypothalamus,inflammatory damage (tuberculosis,sepsis) of hypophysis, inherent aplasia and hypoplasia can lead to development of panhypopituitarity. The most frequently is disordered gonadotropic function of hypophysis and secretion of STH with following development ofinsufficient secretion of ТТH, ACTH and prolactine.
Disturbances of functions of hypophysis.Hypofunction of adenohypophysis (hypopituitaritism) Partial hypopituitarityis the disorder of formation of separate hormones of adenohypophysis (not all). The following variants of partial hypopituitarity are described: • 1) Hypophysar nanism (dwarfishness) - deficiency of STH; • 2) Secondary hypogonadism - deficiency of FSH and LH; • 3) Secondary hypothyrosis - deficiency of TTH; • 4) Secondary hypocorticism - deficiency of ACTH The insufficiency of STH results to development of hypophysar dwarfishness, or nanism and appears by such disorders: • 1) decrease of intensity of protein synthesis that leads to delay and stop of growth (more than 30 % from average) and development of bones, internal organs, muscles. • 3) fallout of fat mobilizing action with tendency to obesity.
Disturbances of functions of hypophysis.Hypofunction of adenohypophysis (hypopituitaritism) The insufficiency of ACTH leads to secondary partial insufficiency of adrenal cortex. The glucocorticoid function suffers mainly. Mineralocorticoid function practically does not vary. Insufficiency of TTH causes secondary decrease function of thyroid gland and development of secondary hypothyrosis symptoms. In case of primary hypofunction of thyroid gland the introduction of TTH can restore its function. Insufficiency of gonadotropic hormones results in decrease of ability of Sertoli cells to accumulate androgens and oppression of spermatogenesis and ability to impregnation in men. In case of defect of LG hormone the function of Leidig’s cells is infringed, the formation of androgens ceases and develops eunuchoidism with preservation of partial ability to impregnation, as the process of spermatozoids maturing does not stop.
Hyperfunction of adenohypophysis (hyperpituitarism) The main reason of hyperpituitarism is development ofbenign tumor – adenoma of endocrine cells. There are two groups of adenomas. • 1. Eosinophilic adenoma, develops from acidophilic cells of adenohypophysis forming STH. Clinically hyperproduction of STH appears by giantism (if adenoma develops in children and young people before closing of epiphysar cartilages) and acromegalia (in adult). Giantism is characterized by the proportional increase of all body components. Acromegalia appears by increased growth of hands, legs, chin, nose, tongue, liver, kyphoscoliosis. Besides that increased metabolic activity of STH -hyperglycemia, insulin resistanse, even to development of metahypophysar diabetes, fatty infiltration of liver develop.
The tallest man in the world – Sultan Kosen (2 m 47 sm) • The lowest man in the world – He Pingping (74,61 sm) – died in the last year in Italy
Khagendra Thapa Mager – world smallest man (64 sm growgh, 10 kg weight). Nepal.
Thapa Mager with your parents He is18 years ago
Hyperfunction of adenohypophysis (hyperpituitarism) • 2. Basophilic adenoma, grows from basophilic cells of adenohypophysis which more often produce ACTH. During this the Itsenko-Cushing disease develops. It is characterized by: • а) secondary hypercorticism; • b) strengthened pigmentation of skin. There are tumors which produce other hormones of adenohypophysis less often: TTH, gonadotropic hormones, prolactin, MSH. The increased level of ACTH during this disease is combined with increase of level of other products of proopiomelanocortin.
Hyperfunction of neurohypophysis Their main effects: Vasopressine (antidiuretic hormone) renders the following influence through V1 and V2 receptors: • 1. Act on tubulus contortus distalis and collective tubules of kidneys, strengthens reabsorption of water; • 2.Causes contraction of smooth muscles of blood vessels; • 3. Strengthens glycogenolysis and gluconeogenesis in liver; • 4.Stimulates consolidation of memory traces and mobilization of saved information (hormone of memory); • 5.Endogenic analgetic (depresses pain).
Hyperfunction of neurohypophysis Oxytocinrealizes the next functions: • 1. Stimulates secretion of milk (lactation) causing contraction of myoepithelial cells of small-sized ducts of mammary glands; • 2. Initiates and strengthens contractions of uterus of pregnant woman; • 3. Worsens storing and mobilization of information (amnestic hormone). Redundant secretion of vasopressin arises in tumors of different tissues forming vasopressin, and also in disorders of hypothalamic endocrine function regulation. Its main manifestation is hypervolemia leading to development of stable arterial hypertension.
Hypofunction of neurohypophysis Insufficient production of vasopressin results to development of diabetes insipidus. There are two pathogenetic variants: • Central (neurogenic) during which will a little quantity of vasopressine is formed • Nephrogenic during which the sensitivity of epithelial cells receptors of distal nephron to vasopressin is reduced. The decreasing of water reabsorption in kidneys results to poliuria and decreasing of circulatting blood volume (hypovolemia), falling of arterial pressure and hypoxia. The decrease of oxytocin production appears by disorders of lactation, weakness of labor activity.