Download
1 / 50
530 likes | 891 Views
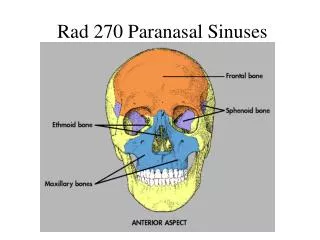
Diseases of the paranasal sinuses Ehab ZAYYAN, MD, PhD. Anatomy. Paranasal sinuses. Cavities found in the interior of the maxilla, frontal, sphenoid and ethmoid bones. The function of the sinuses is to act as resonators of the voice and to reduce the weight of the skull. Paranasal sinuses.

E N D
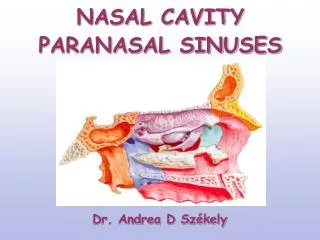
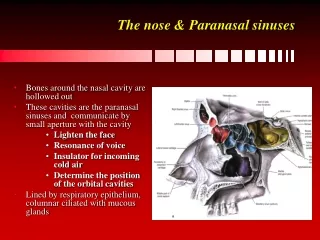
Paranasal sinuses • Cavities found in the interior of the maxilla, frontal, sphenoid and ethmoid bones. • The function of the sinuses is to act as resonators of the voice and to reduce the weight of the skull.
Maxillary sinuses • The maxillary sinus drains into the middle meatus
Frontal sinuses • Two in number • 15 % of humans have a single frontal sinus • 5 % of humans has no frontal sinus. • Each frontal sinus opens into the middle meatus
Sphenoidal sinuses • Two in number • Lie within the body of the sphenoid bone • At the center of the skull • Each sinus opens into the sphenoethmoidal recess → superior meatus
Ethmoidal sinuses • Separated from the orbit via a thin plate called the lamina papracea. • Air cells: 4- 17 (average: 9) in each side • Divided into 2 groups: • Anterior group: opens into the middle meatus • Posterior group: opens into the superior meatus
Relations of the ethmoids: • Anterior: orbit and nasolacrimal duct • Posterior: sfenoid sinus, orbital apex, optic nerve • Lateral: orbit • Superior:skull base
lateral nasal wall • Superior, middle and inferior conchae. • The area below each concha is called meatus: superior, middle and inferior meatus
Embryology • Ethmoid sinuses: 0- 12 y • Frontal sinus: 6- 20 y • Maxillary sinus: 0 - 3 y 7 - 12 y • Sphenoid sinus: 3- 20
Histology • The nasal vestibule is lined with stratified squamous epithelium with vibrissae, sweat glands, and sebaceous glands. • The mucous membrane lines the nasal cavity except the vestibule. There are two types of mucous membranes: 1. Olfactory mucosa 2. Respiratory mucosa
1. olfactory mucous membrane: lines the superior surface of the superior concha and the sphenoethmoidal recess. It also lines the corresponding part of the nasal septum
2. The respiratory mucous membrane: • Pseudostratified ciliated, columnar epithelial cells, goblet cells, and submucosal glands • Its function is to warm, moisten and clean the inspired air. • Warming: venous plaxus in the submucosa • Moisture: mucous by the glands and goblet cells • Ciliary action….
Physiology The mucous membrane consists of two layers: • Gel layer: thick viscous elastic layer • Sol layer: serous layer between the cilia • Daily mucous secretion: 600 – 1800 cc • Contains a lot of substances mainly lysozymes and immunoglobulins.
Ciliary movements: • 50- 300 cilia/ cell • 8-20 beat/ second • The movement is towards the natural ostium not towards the gravity. For maximum ciliary activity: • Humidity: >85% • Temperature: 18- 40 degree C • pH: 7- 8
The sinus mucosa consists of pseudostratified ciliated, columnar epithelial cells, goblet cells, and submucosal glands that produce a protective mucous blanket. • The mucosal blanket traps bacteria and noxious materials, which are carried by ciliary motion to the ostium and into the nose for elimination. • The orientation of the cilia within a given sinus is specific as secretions are propelled towards the natural sinus ostia and from there to the nasopharynx and oropharynx where they are subsequently cleared by swallowing. • This mucosa is similar to that found in the nose and tracheobronchial tree
For normal function • Normal ventilation • Normal drainage • Ciliary movements
Examination of the paranasal sinuses • Palpation • Transillumination • Nasal cavity regular and endoscopic examination • Radiologic examination: - Sinus Water x- ray - Coronal sinus CT
Sinonasal imaging • Plain sinus radiographs: • Sinus opacifications • Air-fluid level • Mass • Fractures
Water view • Best for maxillary sinuses and orbital rims • Blow-out fractures
Computed tomography • Excellent views of the sinuses • Coronal section • Best for osteomeatal complex and ethmoidal disease
MRI • Excellent soft tissue definition • Neoplastic disease evaluation • Fails to demonstrate bone • Expensive • Claustra- phobia
Osteomeatal complex • The most commonly infected structure in the sinuses • Can be obstructed and inflammed easily with even minimal edema • Can not be examined by anterior rhinoscopy but with endoscopy • Can not be evaluated by conventional radiology but needs CT
Factors negatively affecting the mucociliary activity • Dryness of air • Cigarette • Temperature • Hypoxia • Hypercapnia • Hypertonic/ hypotonic fluids • Dehydration • pH changes • Cystic fibrosis • Primary ciliary dyskinesia • Drugs ( phenylphrine, adrenaline, lidocaine, atropine, antihistaminic). • Infections • Anatomic obstruction (septum, turbinate,..) • Foreign body • Nasal polyps
Hypoxia ↓ Vasodilatation Ciliary dysfunctionMucous gland ↓ dysfunction ↓ Stasis ↓ ↓ Transudation Accumulation of thick ← thick fluid secretions in the sinuses ↓ Bacterial growth
Anatomic variations Foreign body Mucociliary dysfunction Allergy Infections Local inflammation ↓ Obstruction of the osteomeatal complex ↓ Sinusitis
Osteomeatal complex obstruction, ↓ Decreased ventilation of the sinuses, Decreased drainage of the sinuses ↓ pO2 decrease, pCO2 increase, mucous stasis ↓ Inflammation and viscous mucous, ciliary movement slowing ↓ Stasis and proteolytic enzymes ↓ Ciliary damage ↓ Anaerobic microrganisms ↓ More damage……
Pathophysiological stages of sinusitis • Initial phase • Ostium obstruction phase • Bacterial phase • Chronic phase
1.Initial phase • Edema and hyperemia of the sinus mucosa • Transudate accumulation and serous fluid • Reversible • If the ostium is not obstructed it resolves spontaneously
2. Ostium obstruction phase • Sinus drainage and ventilation decreases • The secretion becomes thicker and more viscous • Ventilation decreases more, pO2 pressure ↓, CO2 ↑ • A good media for anaerobes develop
3. Bacterial phase • Rapid bacterial growth • Anaerobic bacterial growth • Local inflammation • Viscosity increases • Ciliary activity decreases • If not treated chronic changes start
4.Chronic phase • Immune activities stop • Irreversible changes occur • Mucosal destruction • Ciliary activity stops • The irreversibla changes usually affect some of the mucosa, so if surgery (FESS) is performed, the rest of the mucosa can be saved and start functioning….