Download
1 / 50
520 likes | 936 Views
Comprehensive Approach. Inflammation. Inflammation and repair. Inflammation is fundamentally a protective response Inflammation and repair may be potentially harmful The inflammatory response consists of two main components, a vascular reaction and a cellular reaction.

E N D
Comprehensive Approach Inflammation
Inflammation and repair • Inflammation is fundamentally a protectiveresponse • Inflammation and repair may be potentially harmful • The inflammatory response consists of two main components, a vascular reaction and a cellular reaction
Inflammation and repair • Neutrophils, monocytes, eosinophils, lymphocytes, basophils, and platelets. • Mast cells, fibroblasts, resident macrophages and lymphocytes. • The extracellular matrix
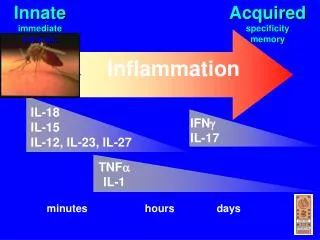
Inflammation and repair • Acute inflammation • Chronic inflammation • The vascular and cellular reactions of both acute and chronic inflammation are mediated by chemical factors
Inflammation and repair Historical Perspective: • (Latin, inflamatio, to set on fire) • The word "inflammation" goes back at least to ancient Egyptian times. “Shem-e-met " : Inflammation and ends in a symbol called a determinative, a "flaming brazier". This brazier is a device heated with fire.
Dr.Maha Arafah: Dr.Maha Arafah:
Inflammation and repair • Leukocyte extravasation • Leukocyte localisation and recruitment to the endothelium local to the site of inflammation – involving margination and adhesion to the endothelial cells
Inflammation and repair • Greek for flame, and indeed an inflamed body part may feel ‘on fire’. In its traditional clinical description, inflammation has four characteristics: calor (heat), rubor (redness), tumor (swelling and dolor (pain).
Inflammation • Overview of Cellular Mechanisms Involved in Acute Inflammation • Chemical Mediators of Acute Inflammation • Examples of Acute Inflammatory Responses • Differences Between Acute and Chronic Inflammation • Examples of Chronic Inflammation • Discussion of Potential Roles of Nutrition in Inflammation
Acute InflammationAcute inflammation is a rapid response to an injurious agent thatserves to deliver mediators of host defense—leukocytes and plasma proteins—to the site of injury. Acute inflammation has three majorcomponents: (1) alterations in vascular caliber that lead to an increase in blood flow; (2) structural changes in the microvasculature that permit plasma proteins and leukocytes to leave the circulation; and (3) emigration of the leukocytes from the microcirculation, their accumulation in the focus of injury, and their activation to eliminate the offendingagent
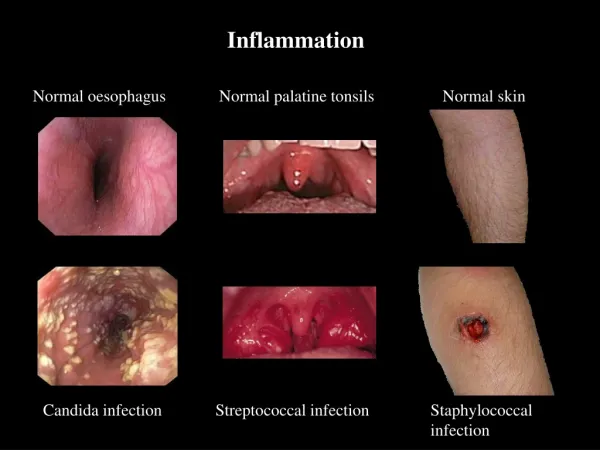
Acute inflammatory reactions aretriggered by a variety of stimuli: • Infections (bacterial, viral, parasitic) and microbial toxins • Trauma (blunt and penetrating) • Physical and chemical agents (thermal injury, e.g., burns or frostbite; irradiation; some environmental chemicals) • Tissue necrosis (from any cause) • Foreign bodies (splinters, dirt, sutures) • Immune reactions (also calledhypersensitivity reactions)
Acute InflammationWhen a host encounters an injurious agent, such as an infectious microbe or dead cells, phagocytes that reside in all tissues try to get rid of these agents. At the same time, phagocytes and other host cells react to the presence of the foreign or abnormal substance by liberating cytokines, lipid messengers, and the various other mediators of inflammation. Someof these mediators act on endothelialcells in the vicinity and promote the efflux of plasma and the recruitment of circulating leukocytes to the site where the offending agent is located.
Acute Inflammation - continuedAs the injurious agent is eliminated and anti-inflammatory mechanisms become active, the process subsides and the host returns to a normal state of health. If the injurious agent cannot be quickly eliminated, the result may be chronic inflammation. The recruited leukocytes are activated by the injurious agent and by locally produced mediators, and the activated leukocytes try to remove the offending agent by phagocytosis.
The vascular phenomena of acute inflammation are characterized by increased blood flow to the injured area, resulting mainly from arteriolar dilation and opening of capillary beds induced by mediators such as histamine. Increased vascular permeability results in the accumulation of protein-rich extravascular fluid, which forms the exudate. Plasma proteins leave the vessels, most commonly through widened interendothelial cell junctions of the venules. The redness (rubor), warmth (calor), and swelling (tumor) of acute inflammation are caused by the increased blood flow and edema.
Circulating leukocytes, initially predominantly neutrophils, adhere to the endothelium via adhesion molecules, transmigrate across the endothelium, and migrate to the site of injury under the influence of chemotactic agents. Leukocytes that are activated by the offending agent and by endogenous mediators may release toxic metabolites and proteases extracellularly, causing tissue damage. During the damage, and in part as a result of the liberation of prostaglandins, neuropeptides, and cytokines, one of the local symptoms is pain (dolor).
Changes in vascular flow and caliber begin early after injury and develop at varying rates depending on the severity of the injury. The changes occur in the following order: • Vasodilation. Increased blood flow is the cause of the heat and the redness. Vasodilation is induced by the action of several mediators, notably histamine and nitric oxide on smooth muscle.• Increased permeability of the microvasculature. • Stasis. The loss of fluid results in concentration of red cells in small vessels and increased viscosity of the blood.
A hallmark of acute inflammation is increased vascular permeability leading to the escape of a protein-rich fluid (exudate) into the extravascular tissue. The loss of protein from the plasma reduces the intravascular osmotic pressure and increases the osmotic pressure of the interstitial fluid. Together with the increased hydrostatic pressure owing to increased blood flow through the dilated vessels, this leads to a marked outflow of fluid and its accumulation in the interstitial tissue. The net increase of extravascular fluid results in edema.