Download
1 / 20
200 likes | 494 Views
DAP RWANDA. Development Assistance Program A multisectoral approach to livelihood security in Rwanda. USAID funded. FY 2005- FY 2009. Overall goal: improve livelihood security for 700, 000 households in Rwanda Partners: WV/R, ADRA and FHI. Country overview. Population: 9 million

E N D
DAP RWANDA • Development Assistance Program • A multisectoral approach to livelihood security in Rwanda. • USAID funded. • FY 2005- FY 2009. • Overall goal: improve livelihood security for 700, 000 households in Rwanda • Partners: WV/R, ADRA and FHI
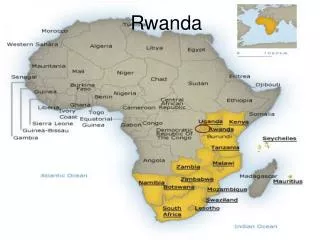
Country overview • Population: 9 million • Population density- 336 persons per square km • 5 provinces, 30 districts. • Each district made up of sectors, each sector made up of cells. • DAP coverage- Northern province: Gicumbi, Gakenke, Musanze; Eastern province: Bugesera; Southern province: Nyamagabe and Nyaruguru.
Situational analysis • Livelihood of rural Rwanda is largely dependent on subsistent farming (over 90%) • Causes of livelihood insecurity/malnutrition are numerous and often intricately related: • Mainly can be categorized into: • Factors leading to low agricultural productivity • Land scarcity from high population density (average of 0.7 hectares per capita) • Soil erosion from unfavourable topography, deforestation and poor land practices (Rwanda between 1,000 and 4500 meters, 50% reduction of forest areas post genocide) • Poor climactic conditions: erratic rainfalls leading to drought and flooding. • Limited agricultural information, knowledge and skills (poor quality extension services)
Situational analysis II • Factors related to limited market and economic opportunities • Limited market access: poor rural roads network, lack of transportation and small size of local market. • Lack of collective bargaining power and little influence on market forces. (smallholder farmers poorly organized) • Lack of capital and access to credit: limited financial management skills and unfavourable borrowing terms. • Factors related to the depletion of human capital • High OVC and HIV burden (Rwanda prevalence- 3%) leads to workforce depletion and reduction of household earnings. • Malnutrition and HIV/AID mutually aggravate one another and impact negatively on productivity. Productivity loses to malnutrition is approximately 10% of life time earnings (World Bank)
DAP Objectives • A multisectoral approach with interacting sectors. • Increased household agricultural Production and Productivity through: Improved farming systems, strengthen soil conservation practices, diversification of assets base. • Increased Economic Opportunities in Rural Areas through improved market access and efficiency • Improved health and nutrition for women, children and vulnerable groups and reduction of risk andimpact of HIV/AIDS • Improved governance through increased positive interaction among diverse groups of people.
HIV Sector • Objective: reduce risk of and mitigate the impact of HIV/AIDS • Dissemination of Behaviour change messages: • Health education for PLWHA on nutrition and hygiene • Disseminating HIV prevention messages among farmers. • HIV prevention education to women’s group. • Supplementary food ration for PLWHA • Family ration consisting of: (CSB, fortified bulgur and vegetable oil) • PLWHA in need of food assistance surpass resources: criteria used include ARV status, children, lactating mothers and BMI<18. • PLWHA kept on food ration for minimum of 6 months
Nutrition and Health sector • Objective: improved nutritional status of targeted vulnerable groups: • Growth monitoring and selection of malnourished children for supplemental feeding. • Provision of supplementary ration and vitamins for nutritional recuperation of target children. • Training mothers/foster parents and nutrition and health workers on PD/Hearth model and Care group concept. • Nutritional rehabilitation through the PD Hearth approach. • Mothers care group to improve infant and young child feeding (FHI) • Sensitive community on malaria prevention. • Mothers provided with improved vegetable seeds • Mothers trained in bio-intensive kitchen gardens
Livelihood sector • Improved farming systems • Promote the use of improved varieties of key crops • Promote best cultural practices • Enhance crop diversification • Strengthen research-extension-farmer linkages • Strengthen soil conservation practices • Control soil degradation on hillside (Land terracing through the FFW program) • Train farmers in environmentally sound practices • Promote tree panting and agro-forestry practices • Promote the use of energy saving stove. • Household food security enhanced through diversification of assets base. • Promote bio-intensive market gardening • Promote bio-intensive farming and small animal rearing.
Inter-sectoral integration • For for Work (FFW): land terracing increases land productivity in the long term but increases household food security in the short term. • PLWHA included in FFW program: reduces socio-economic impact of HIV/AIDS. • PLWHA trained in non-labour intensive (context specific) farming methods: kitchen gardens, planting in sacks: sustains immediate gains from food supplementation programs. • Farmers given HIV prevention education: leads to long term productivity gains. • Mothers of malnourished children given improved vegetable seeds and trained in bio-intensive kitchen gardens: sustains nutrition rehabilitation programs.
Integrated Nutrition / MCH / Food Security Framework Nutrition / MCH Ag Marketing / Production Value-chain approach Clinic / Health Center Community Health Promoters Functions Nutrition Rehab. Rally Point Link to markets, technologies, credit Training in business skills, access to markets & credit Safety nets (food for work, etc.) Retail Associations, cooperatives, mothers groups Positive deviant leaders Health extension workers MothersCare Groups (15) Wholesale Growth Monitoring,Screening Malnourished under 5s) Under 5s Preg./Lac. PLWA OVCs Households (10) Assembly Individuals Entrepreneur start-up support Families Kitchen, community, health center gardens • Kitchen gardens • Small animals • Fruit & vegetables Farmer field schools Production Multiplication of improved varieties On farm trials, demonstrations CTC (Severely) Hearth (moderately) Seed fairs, vouchers, etc. Input Supply gardens Public Sector Private Sector
Trained 3473 farmers on bio-intensive gardening and 3153 on organic farming (FY 07 target for both was 2400) Trained 11, 895 beneficiaries on HIV prevention. Trained 16818 mothers on key health and nutrition lessons. 36% of targeted farmers adopting bio-intensive gardening (FY 07 target- 20%) 40% of targeted farmers adopting organic farming practices. (FY 07 target 25%) MCH Outcomes: (Mid-term survey results) 91% of mothers adopting proper hand washing behaviour (baseline 19%) Stunting rate reduced from 47.6% to 40% Underweight (weight for age) reduced from 27.7% to 22%. Number of men and women 15-49 who can mention at least 2 ways of preventing HIV/AIDS- 95% (baseline- ) Key Achievements FY 07
Outcomes 2 (FGDs) • Nutrition knowledge and practices • All mothers knew to exclusively breastfeed their infants for 6 months and then introduce complimentary foods, continue to offer breast milk on demand for up to 24 months • Had or were breastfeeding their infants and some for up to 24 months • Knew the importance of providing dense complementary foods using local foods and could identify local nutritious foods • Knew to continue to feed their children during illnesses.
Outcomes 3 (FGDs) • Health knowledge and practice among mothers: • 97% participated in the growth monitoring program • 84% received vitamin A • 85% received deworming • All had their children sleep under bed nets • All had at least 4 prenatal visits and know the importance of skilled attendants for labour and delivery. • All had their children fully immunized. • All could state at least 3 ways that HIV is transmitted
My name isNyirabashongore Amerberga of 37 years old. I’m married with 2 kids. My husband died in 2000, and after his death, I used to get sick without knowing the cause. After being trained, I was tested and found that I’m positive in 2006 and I decide to join association. Before getting food, I washaving 30 CD4 (in September 2006). In March 2007 she had CD4153, and now she is having CD4 197. Outcomes 4
Key Challenges • Applying criteria for including PLWHA into food supplementation programs in the midst of huge needs. • Therapeutic feeding centres sometimes non-existent. • Resource/budget constraints limiting income generating activities for PLWHA graduated from food supplementation programs. • Removal of Rwanda from the list of high priority countries. • Slow sales of monetization commodities and hence cash flow problems • Integration of the DAP with other WVR programs. • On-going AID Reforms and the need to make adjustments