Download
1 / 23
240 likes | 603 Views
Presented by: Praharsha R. Menon, MD Emory Family Medicine 10/21/2010. Osteoporosis: SCREENING AND TREATMENT. DEFINITION:. Thick outer shell and a strong inner mesh filled with collagen (protein), calcium salts and other minerals .

E N D
Presented by: Praharsha R. Menon, MD Emory Family Medicine 10/21/2010 Osteoporosis: SCREENING AND TREATMENT
DEFINITION: • Thick outer shell and a strong inner mesh filled with collagen (protein), calcium salts and other minerals A progressive systematic skeletal disease characterized by low bone mass and micro-architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture
A FEW POINTERS… • Prevalence: 15 million in women and 3 million in men
RISK FACTORS For osteoporosis For fragility fractures • Female gender • Increased age • Hypogonadism • White race • Low body mass index • Family history • Tobacco use • History of fracture • Chronic glucocorticoid or anticoagulant use • Endocrinopathies • High bone turnover and microarchitectural changes • History of falls • Poor physical condition • Dementia • Impaired vision • Environmental hazards • Current use of benzodiazepines or anticonvulsants www.aafp.org/afp
SCREENING GUIDELINES • USPSTF(United States Preventive Services Task Force) • NOF (National Osteoporosis Foundation) • ISCD (International Society of Clinical Densitometry
USPSTF: SCREENING • Routine screening: • F >/= 65 yo • F>/= 60 yo if at increased risk for osteoporotic fractures B • No recommendation for or against routine screening in postmenopausal F <60 yo or in F < 60-64 yo who are not at increased risk for osteoporotic fractures C • All men >/= 70 yo (NOF, ISCD) C
DEXA SCAN • Dual-Energy X-Ray Absorptiometry • Uses: • diagnosis of low bonedensity • prediction of fracture • WHO definitions of osteoporosis and osteopenia • Monitoring BMD in patients being treated for osteoporosis • Low radiation, noninvasive, fast
Which Skeletal Site(s) Should BeMeasured? Every Patient: • Spine : L1- L4 • Hip – Total Hip – Femoral Neck Some Patients: • • Forearm (33% radius, • 1/3 radius) • – If hip or spine cannot be • measured • – Hyperparathyroidism • – Very obese NOF: uses femoral neck measurement only ISCD: uses both hip and spine measurements The lowest score across sites determines the diagnosis
WHO classification with a T-score cannot be applied to premenopausal women, men under age 50, or children (Z score used) • Best predictor of osteoporotic fracture: BMD
FRAX: • Measures probability of fracture in the next 10 years • WHO task force led by John Kanis used data from nine epidemiological studies from the US, Europe, Australia, and Asia to determine risk factors for osteoporotic fracture • Independent of BMD • 11 risk factors can be used +/_ BMD by DEXA
RISK FACTORS BY FRAX • Age (between 40 and 90 years) • Sex (female and male) • Weight in kg • Height in cm • Previous fracture while an adult • Parental fracture (mother or father) • Smoking (current) • Alcohol (3 or more drinks daily) • Systemic steroids (5 or more mg prednisone or more for 3 or more months, current or past history) • Rheumatoid arthritis • Secondary osteoporosis
EVALUATION FOR SECONDARY OSTEOPOROSIS • CMP including ALP, liver fxn, kidney fxn • Calcium • CBC • TSH • Total testosterone (men) • 25-hydroxyvitamin D (men) Additional tests (based on level of severity of osteoporosis or clinical suspicion of underlying disease): • Estradiol (pre- or perimenopausal women) • Intact PTH • Serum protein electrophoresis • 25-hydroxyvitamin D (women) www.aafp.org
US TREATMENT THRESHOLD BY FRAX • 10 - year probability of hip fracture > 3 % or • 10 - year probability of major osteoporotic fracture > 20%
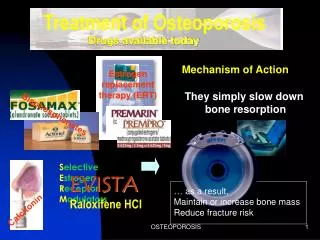
TREATMENT • Antiresorptives: Alendronate, Risedronate, Ibandronate, Zoledronic acid, Raloxifene, Calcitonin, Estrogen • Anabolic (bone forming): Teriparatide
TREATMENT INDICATIONS: NOF • Hip or vertebral fracture • T-score -2.5 or less at femoral neck (or total hip) or spine • T-score between -1 and -2.5 and a 3% (or greater) 10-year probability of hip fracture or a 20% (or greater) 10-year probability of major osteoporotic fracture, using FRAX
ALSO… • T - score between -1 and -2.5 and : a disease or medication associated with osteoporosis prior fracture (other than hip or vertebral) and T - score between -1 and -2.5
MEDICATIONS TREATMENT • Alendronate • Risedronate • Ibandronate PO and IV • Zoledronic acid • Raloxifene • Teriparatide • Calcitonin PREVENTION • Alendronate • Risedronate • IbandronatePO • Raloxifene • Estrogen
NON-PHARMACOLOGIC TREATMENT • Fall prevention • Vitamin D: • 800 to 1,000 IU daily for persons 50 years and older (NOF) • Documented vitamin D deficiency: oral vitamin D2 50,000 IU weekly for 8 weeks followed by a maintenance dosage of 50,000 IU every two to four weeks or oral cholecalciferol (vitamin D3) 1,000 IU once daily • Calcium: at least 1200 mg daily
PREVENTION • Adequate amounts of calcium • Adequate amounts of vitamin D • Regular exercise • Lifestyle modification • Screening in appropriate age groups
REFERENCES • Diagnosis and Treatment of Osteoporosis: Sweet MG, et al. American Family Physician Feb., 2009 • Osteoporosis: Part I. Evaluation and AssessmentL South-Paul JE, et al. American Family PhysicianMar. 1, 2001 • www.uspreventiveservicestaskforce.org • Mayoclinic.com