Download
1 / 36
360 likes | 548 Views
WHEN SCIENCE CATCHES THE EYE. D. BALASUBRAMANIAN L. V. PRASAD EYE INSTITUTE HYDERABAD 500034, INDIA. IN THIS TALK, WE SHALL FOCUS LESS ON BIOLOGY AND CONCENTRATE MORE ON WHAT POLYMER CHEMISTRY, MATERIAL SCIENCE, OPTICS AND ENGINEERING SCIENCES HAVE BEEN CONTRIBUTING TO VISION SCIENCE.

E N D
WHEN SCIENCE CATCHES THE EYE D. BALASUBRAMANIAN L. V. PRASAD EYE INSTITUTE HYDERABAD 500034, INDIA
IN THIS TALK, WE SHALL FOCUS LESS ON BIOLOGY AND CONCENTRATE MORE ON WHAT POLYMER CHEMISTRY, MATERIAL SCIENCE, OPTICS AND ENGINEERING SCIENCES HAVE BEEN CONTRIBUTING TO VISION SCIENCE. FOCUS ON AREAS SUCH AS PRESBYOPIA, MYOPIA, DIABETIC RETINOPATHY, “SMART CONTACT LENSES” AND THE BIONIC EYE. AND WONDER ABOUT WHAT TODAY APPEAR TO BE SOME SEEMINGLY IMPOSSIBLE THINGS TO DO.
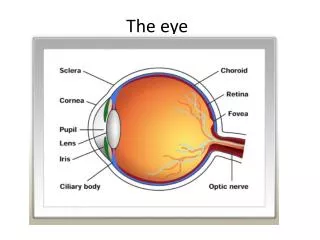
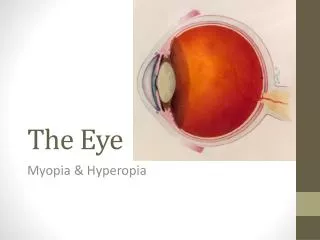
LIGHT IS REFRACTED BY THE CORNEA AND THE LENS AND FOCUSSED ON THE RETINA; THE IRIS CONTRACTS AND EXPANDS TO LET IN THE APPROPRIATE LEVEL OF INCOMING LIGHT THROUGH THE PUPIL
80% of focusing is by cornea, 20% by the lens, but the refractive index of cornea does not vary as much as that of the lens does; accommodation is done by the lens
Concept Overview • Ciliary muscle contraction • Decrease in anterior chamber depth • Increase in lens thickness • changed anterior and posterior radius of curvature
WITH AGE, THE LENS BECOMES STIFFER AND ACCOMMODATES LESS- CLILIARY MUSCLES ARE NOT ABLE TO DEFORM THE LENS TO ADJUST TO THE CORRECT FOCAL LENGTH- DIOPTER VALUE (1/FL, in M); PRESBYOPIA HENCE THE NEED FOR READING GLASSES In 1784, Ben Franklin developed bifocal glasses. He was getting old and was having trouble seeing both up-close and at a distance. Getting tired of switching between two types of glasses, he devised a way to have both types of lenses fit into the frame. The distance lens was placed at the top and the up-close lens was placed at the bottom.
By this means, as I wear my spectacles constantly, I have only to move my eyes up or down, as I want to see distinctly far or near, the proper glass being always ready. This I find more particularly convenient since my being in France, the glasses that serve me best at table to see what I eat, not being the best to see the faces of those on the other side of the table who speak to me; and when one’s ears are not well accustomed to the sounds of a language, a sight of the movements in the features of him that speaks helps to explain, so that I understand French better by the help of my spectacles.” BIFOCALS ARE NOT THE ONLY THE INVENTION OF BENJAMIN FRANKLIN! HE WON THE CONTRACT TO PRINT CURRENCY NOTES IN PENNSYLVANIA, INVENTED A MORE EFFICIENT STOVE, MADE AN ELECTRICAL BATTERY, THE LIGHTNING ROD, FOUNDED THE AMERICAN PHILOSOPHICAL SOCIETY, INITIATED THE FIRST CENSUS OF AMERICA……
WHAT CAN BE DONE TO RID OF BIFOCALS? WHAT CAN SCIENCE OF TODAY DO TO HELP? CAN WE GET RID OF NEAR VISION GLASSES? Presbyopic Correction • ACCOMMODATIVE INTRAOCULAR LENSES • REPLACE THE LENS BY POLYMER GEL • POLYMER CHEMISTRY COMES TO HELP • PMMA, HYDROXYSILANES, HYDROGELS
Accommodation: Biomechanics • Structures involved in accommodation • Crystalline lens; Ciliary muscle; Choroid; Suspensoryzonules • Innervation • Parasympathetic • Edinger-Westphal (EW) nucleus
Accommodative IOL: Crystalens • Crystalens manufactured by Eyeonics (B & L) • Plate-haptic lens has a hinged design, permitting forward movement of the haptics as a result of pressure changes in the vitreous cavity
Single-Optic A-IOL’s Crystalens translating A-IOL 1-CU translating A-IOL Dick, 2005
Enhanced Single Optic Designs Crystalens AT 45 (Eyeonics Inc.) 12 month phase II clinical trial: the only FDA- approved accommodating IOL Plate haptic silicone multi-piece IOL 263 patients with one-year follow-up* 90% achieved near VA of 20/40 or better 25% : 20/32 or better However, inadequacy: single optic design of the lens; inadequate accommodation
A Dual Optic Accommodating IOL High + Power Anterior Haptics (3x) Low - Power Posterior
Concept Overview • Use natural forces of ciliary processes • Change optic-to-optic separation to vary vergence point • Requires in-the-bag implantation • Accommodated • Distance
Smart Lens (H. Fine) • The “SmartLens” concept: upon hydration, the polymer rod swells to a disc lens 9.5 mm in diameter and 2–4 mm thick, within approximately 30 s. • a: Schematic; b: soft and compressible disc lens
Injectible A-IOLs Haefliger & Parel, 1986
Phaco-Ersatz 2009 Apply MCV Incision Lavage Completed Injection Capsulorhexis 1 19 Curing Extraction
Unresolved Problems • Achieving emmetropia in relaxed state • Ideal polymer with optimum accommodation & biocompatibility • Surgical technique for hard cataract • PCO • Can chemistry/physics/material science help here? Need help!
WHY THIS OBESSION WITH MYOPIA AND PRESBYOPIA? Because they are endemic in many parts of Asia, and India. Myopia: China: 31.7 % of primary school children and 82.7 % of University students have impaired vision. 90% of youngsters in Singapore and Taiwan become myopic before they reach class X. We do not have such estimates yet in India, but we estimate that 0.17% of children in India are blind (<6/60); of these 33% are due to refractive errors. Means >1.3 million are myopic. Genetics, and ‘near work’ are two factors associated with myopia
Presbyopia: Over 77 million Indians are over 60 years of age. This number is expected to rise to 117 million by 2025. But presbyopia hits people already by the age of 40; Nirmalan et al. have estimated that 55% of people studied (age 47.5 ± 13 years) in Andhra Pradesh are presbyopic (at least +I D correction); females had a slightly higher odds (OR 1.4), rural residence OR 1.5, myopics OR 1.6 and hyperopia OR 3.6. Translated to the whole of India, this becomes an epidemic.
CORNEAL ONLAYS TO REDUCE MYOPIA PROGRESSION SLICE A SMALL LAYER OF THE CORNEAL OUTER SURFACE USING A SPECIAL BLADE, INSERT A VERY THIN IMPLANTABLE LENS, AND LEAVE IT THERE. THIS SHOULD CORRECT THE REFRACTIVE ERROR. IF NEED BE, THE LENS CAN BE REMOVED AND REPLACED BY ANOTHER
Epithelium Epithelium Stroma Stroma Lens Lens Quite safe and biocompatible Inlay ↓ 1 m↑, 12 m↓ after inlay Onlay ↑ Onlay, hardly visible Flatten the cornea, lift a chosen thickness of the epithelium or the stroma, insert a thin refractive plastic lens, and correct the refractive error; lens stays for even, or can be replaced; Inlay used only to check biocompatibility. Onlay is under trial to check long term stability of refractive power. ↑
A CORNEAL ONLAY BEING DONE BY Drs. PRAVIN K. VADLAMUDI and ASHIK Md
MYOPIA AFFECTS THE PERIPHERAL RETINA AS WELL. WE MISS THIS DUE TO RETINAL RESOLUTION, AND THE CURVATURE OF THE EYE LENS, WHICH FOCUSES ON THE FOVEA, AND OF THE EYE ITSELF; WE NEED TO LOOK AT THE PERIPHERAL REGIONS OF THE FOVEA AS WELL. BUT CURRENT SPECTACLE LENSES OR CONTACT LENSES DO NOT TAKE THIS INTO ACCOUNT; NEED RE-DESIGNED AND RE-GROUND LENSES. a b → See the myopia (a) and hyperopia (b) in retina, even as the fovea is on focus Prototype spectacles that takes care of peripheral retinal focus Lundstrom L, Mira-Agedelo A. Artal P. Peripheral optical errors and their change with accommodation differ between emmetropic and myopic eyes. J. Vision, 2009
ADAPTIVE EYEGLASSES Invented by Dr. Josh Silver of Oxford Univ., this involves the use of transparent silicone oil, whose amount can be adjusted by the use as per needs. From the original (top left), it has improved to the more convenient one (left). Being tried with over 40,000 users in Ghana, this will be taken up by WHO
WHAT ABOUT THE CORNEA? MILLIONS ACROSS THE WORLD NEED CORNEAL REPLACEMENT, AND THE NUMBER AVAILABLE FROM DONORS IS FAR LESS. WHY NOT MAKE AN ARTIFICIAL CORNEA? MUST BE COMPATIBLE WITH THE UNDERLYING/SURROUNDING TISSUE; TRANSPLANTABLE, ACCEPTABLY REFRACTIVE, FLEXIBLE, NON-ABRASIVE, LONG-LASTING, HYDRATED, OXYGEN- PERMEABLE POLYMERS- BIO OR SYNTHETIC APPEAR POSSIBLE RECOMBINANT HUMAN COLLAGEN, PLL-PLGA COPOLYMER, COPOLYMER OF PERFLUOROALKYLVINYL ETHER + TETRAFLUOROETHANE, N-ISOPROPYL ACRYLAMIDE COPOLYMER, TYPE 1 COLLAGEN, WITH POLYVINYL ALCOHOL COPOLYMER COAT, POLY-HYDROXYETHYL METHACRYLATE (PHEMA) By far, the most promising seems to be from Dr. May Griffith, OHRI, Canada; we are trying it at LVP
THE VITREOUS HUMOR TRANSPARENT GEL BETWEEN THE LENS AND ATTACHED TO THE RETINA. WITH AGE, THE VITREOUS GEL LIQUEFIES, AND SEPARATES FROM THE RETINAL SURFACE (POSTERIOR VITREOUS DETACHMENT, PVD). THIS IS GOOD, SINCE PVD DECREASES THE CHANCES OF A DISORDER CALLED PROLIFERATIVE DIABETIC RETINOPATHY, WHERE NEW BLOOD VESSELS FORM AND CAUSE HEMORRHAGE, AS THEY PEEL OFF Normal proliferative ←→ IN DIABETICS, WE WOULD LIKE TO HASTEN PVD, SO THAT RETINOPATHY DOES NOT OCCUR- NO PEELING BASED HEMORRHAGE. SO, NEED ENZYMES THAT RELEASE AND LIQUEFY THE VITREOUS. WE ARE CURRENTLY CLINICALLY TRYING THE PRODUCT “VITREOSOLVE”, BUT NEED NEW IDEAS AND PRODUCTS- HELP FROM COLLEAGUES
TURN NOW TO THE RETINA WHILE BIOLOGY IS TRYING HARD TO ADDRESS RETINAL DISORDERS, ELECTRONICS IS TAKING OVER- THE BIONIC EYE
Retinoblastoma, cancer in the eye- rampant in children in India: treatment by surgery and using carboplatin. Extreme cases, enucleation of the eye. Dosage difficult, as also the actual concentration reaching the site. We have tried encapsulating the drug in PAMAM dendrimers, and delivering it periocularly as also sub-conjunctivally. Are there better ways? Better nano- materials to or other delivery vehicles? → Dr. S. G. Honavar carboplatin PAMAM dendrimer
Camera on the glasses sees image; signals sent to hand-held device; processed information sent back to glasses and transmitted to a receiver under the surface of the eye; receiver sends information to the electrodes in the retinal implant, and the stimulated retina sends information to the brain. Partial visual recovery.
Professor Mark Humayun, earlier at Johns Hopkins, now at USC Los Angeles: “It’s amazing, even with 16 pixels, or electrodes, how much our first six subjects have been able to do”; the newer implant has a higher resolution, with 60 pixels. The pixel number will increase upon experience; currently about 75 subjects Have volunteered for the trial. So, will there be a contact lens retinal implant? Not too far off!
EVEN MORE DARING QUESTIONS Gene delivery using nanomaterials? Eye drops that can reach the retina? Tear fluid as a diagnostic material?? Re-engineer taste bud cells to repair the retina? Transplant an entire donor eye Contact lens as a navigator?
Contact lens turns James Bond! BabakParviz, UW Seattle- incorporates electronic circuitry into a plastic lens, including LEDs for ‘on eye’ displays, radio for wireless communication, antenna for collecting power from a cell phone in the pocket. Useful for GPS, direction navigation, and to find quickest route to a target- military and security/spy use.