Download
1 / 33
400 likes | 1.33k Views
ATHEROSCLEROSIS. Dr. Gehan Mohamed Dr. Abdelaty S hawky. Learning objectives. Definition of arteriosclerosis and mention the three patterns of it? Mention definition, risk factors, gross morphology, and common sites of atherosclerosis?

E N D
ATHEROSCLEROSIS Dr. Gehan Mohamed Dr. Abdelaty Shawky
Learning objectives • Definition of arteriosclerosis and mention the three patterns of it? • Mention definition, risk factors, gross morphology, and common sites of atherosclerosis? • Discuss microscopic picture of atherosclerosis plaque? • Mention complications of atherosclerosis? • Discuss pathogenesis of atherosclerotic plaque formation?
Endothelial cells • Single cell-thick, continuous lining of the entire cardiovascular system, collectively called the endothelium. • Endothelial structural and functional integrity is fundamental to the maintenance of vessel wall homeostasis and normal circulatory function.
Smooth muscle cells • SMCs are predominant cellular element of the vascular media • SMCs are responsible for vasoconstriction and dilation in response to normal or pharmacologic stimuli. • SMCs are important elements of both normal vascular repair and pathologic processes such as atherosclerosis
Arteriosclerosis Arteriosclerosis literally means "hardening of the arteries”. It is a term for thickening and loss of elasticity of arterial walls. Three patterns are recognized: 1. Atherosclerosis: the most frequent and important pattern. 2. Mönckeberg medial calcific sclerosis: is characterized by calcific deposits in muscular arteries in older people. 3. Arteriolosclerosis:affects small arteries and arterioles. Is seen with hypertension and diabetes mellitus.
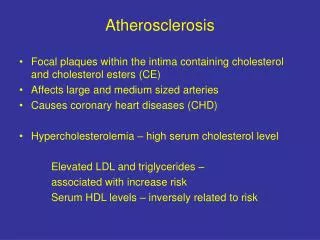
Atherosclerosis Generalized, degenerative arterial disease characterized by patchy thickening of the intima by atheromas, which protrude into and obstruct vascular lumens and weaken the underlying media.
* Gross and microscopic morphology: 1. Fatty spots: are the earliest lesion of atherosclerosis as multiple yellow, flat spots less than 1 mm in diameter. They are composed of lipid-filled foam cells. 2. Fatty streaks:fatty spots coalesce into elongated streaks, 1 cm long or longer. They contain T lymphocytes and extracellular lipid in smaller amounts than in plaques. They are not significantly raised and thus do not cause any disturbance in blood flow.
Fatty streak—a collection of foam cells in the intima Photomicrograph of fatty streak in an experimental hypercholesterolemic rabbit, demonstrating intimal macrophage-derived foam cells ( arrow). Aorta with fatty streaks ( arrows). Slide 12.9
3. Atheroma or atheromatous plaque: consists of raised patches within the intima, having a soft, yellow, core of lipid (mainly cholesterol and cholesterol esters), covered by a firm, white fibrous cap. * Microscopically: Atherosclerotic plaques have three principal components: 1. Cells, including smoth muscle cells (SMCs), macrophages, and other leukocytes 2. Extracelularmatrix(ECM), including collagen, elastic fibers, and proteoglycans 3. Intracellular and extracellular lipid . These components occur in varying proportions.
The previously mentioned components are arranged in these layers : 1. Fibrous cap: in the top composed of SMCs and relatively dense ECM, macrophages, and lymphocytes. 2. Necrotic core: Deep to the fibrous cap , containing cholesterol clefts, necrotic debris from dead cells, foam cells and fibrin.
- Foam cells are large, lipid-laden macrophages derived from blood monocytes, but SMCs can also imbibe lipid to become foam cells.
Gross views of atherosclerosis in the aorta. A. Mild atherosclerosis composed of fibrous plaques, one of which is denoted by the arrow. B. Severe disease with diffuse and complicated lesions. Slide 12.7
* The common sites: • abdominal aorta • coronary arteries • the popliteal arteries • the internal carotid arteries • the vessels of the circle of Willis.
* Complications: 1. Rupture, ulceration, or erosion of the luminal surface of atheromatous plaques. 2. Cholesterol emboli or atheroemboli. may occur after rupture of atheromatous plaque that induce thrombus formation which may be fragmented into microemboli.
3. Hemorrhageinto a plaque may be initiated by rupture of either the overlying fibrous cap or the thin-walled capillaries that vascularize the plaque. A contained hematoma may expand the plaque or induce plaque rupture.4. Thrombosis usually occurs on disrupted lesions (those with rupture, ulceration, erosion, or hemorrhage) and may partially or completely occlude the lumen.
5. Aneurysm: is abnormal dilatation of the arterial wall which is induced by atrophy of the underlying media, with loss of elastic tissue, causing weakness, and potential rupture 6. Calcifications: Atheromas often undergo calcification.
* Atherosclerosis: Major Risk Factors: I. Non-modifiable: • Increasing age • Gender • Family history • Genetic abnormalities
II. Potentially modifiable • Hyperlipidemia. • Hypertension. • Cigarette smoking. • Diabetes.
III. Uncertain risk factors: • Obesity. • Physical inactivity. • Stress ("type A" personality). • Postmenopausal (estrogen deficiency). • Alcoholism. • Hardened (trans)unsaturated fat intake.
Lipoproteins and atherosclerosis: • Some types of lipoproteins promote atheroma formation such as Low-density lipoproteins (LDLs),Very-low-density lipoproteins (VLDLs),Chylomicrons. • But other types such as high density lipoproteins (HDLs) help to protect from atherosclerosis by collecting cholesterol from other lipoproteins and transporting it to places where it can be utilized by the cells
* Pathogenesis of atherosclerosis: Response to injury hypothesis: It considers atherosclerosis to be a chronic inflammatory response of the arterial wall initiated by injury to the endothelium.
1. Chronic endothelial injury induced by: • Hypertension. • Hyperlipidaemia. • Cigarette smoking. • Viruses. • Immune reactions….
2. Adhesion of blood monocytes to the endothelium, followed by their migration into the intima and their transformation into macrophages and foamcells. 3. Adhesion of platelets to the exposed sub-intimal collagen. 4. Release of mitogenic growth factors from activated platelets and macrophages, that cause migration of SMCs from media into the intima
5. Proliferation of smooth muscle cells in the intima, and elaboration of extracellular matrix, leading to the accumulation of collagen and proteoglycans 6. Enhanced accumulation of lipids both within cells (macrophages and SMCs) and extracellularly.
Chronic endothelial “injury” theory Slide 12.13
How to Make an Atheroma 2 Endothelial dysfunction Monocyte adhesion and emigration
How to Make an Atheroma 3 Macrophage activation Smooth muscle recruitment
5, Well-developed plaque. Slide 12.17