Download
1 / 51
530 likes | 778 Views
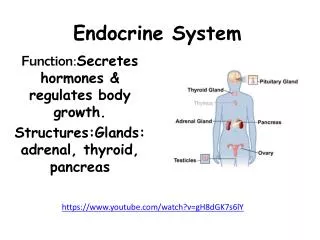
Endocrine System. PTA 120 Pathophysiology Day 15. Objectives . Discuss anatomic structures and physiologic processes related to the endocrine system. Discuss physical effects of aging on the endocrine system. Define endocrine pathological conditions including signs and symptoms of each:

E N D
Endocrine System PTA 120 Pathophysiology Day 15
Objectives • Discuss anatomic structures and physiologic processes related to the endocrine system. • Discuss physical effects of aging on the endocrine system. • Define endocrine pathological conditions including signs and symptoms of each: • Hyperpituitarism • Hyperthyroidism • Hypothyroidism • Hyperparathyroidism
Objectives • Addison’s Disease • Cushing’s Disease • Diabetes Mellitus • Obesity • Discuss how endocrine system pathologies can adversely affect function requiring the modification of treatment intervention to protect the patient from worsening the condition and optimize treatment outcomes.
Objectives • Discuss the modifications and precautions that may be required for the treatment of patients with disorders of the endocrine system. • Demonstrate understanding of the PTA’s role in the disease processes.
Textbooks • Pathology for Physical Therapist Assistants, Ch 9 • Physical Therapy Clinical Handbook for PTAs
Why does the pta need to know about the anatomy and physiology of the endocrine system?
The endocrine system maintains homeostasis within the body. When this is disrupted, the patient’s strength and energy will be altered.
Functions of the endocrine system • Chemical control system • Hormonal control though the blood stream • Slow acting system • Insulin example • Hormones control: • Reproduction • Growth and development • Mobilization of body defenses • Maintenance of homeostasis • Regulation of metabolism
Effects of Aging On the Endocrine System From: Stillerman (Ed), Modalities for Massage and Bodywork, Elsevier, St Louis, 2008, in press.
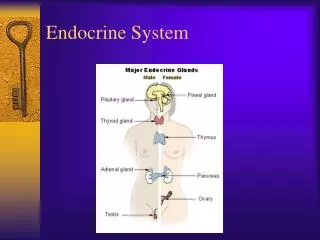
Glands • Endocrine • Ductless glands • Anterior pituitary, thyroid, adrenals, parathyroid • Hormones released into blood • Exocrine • Release products into body’s surface or cavities through ducts
Why does the PTA need to know about diseases and disorders of the Endocrine system? Effects of an endocrine disorder may impact physical therapy treatments for another comorbid diagnosis.
Hyperpituitarism • Description • Enlargement of the pituitary gland • May start in childhood, usually after puberty; gigantism • Adult onset between ages 30 – 50; acromegaly • Prevalence of 4676: 1 million in US
Hyperpituitarism • Etiology • Adenomas • Overproduction of growth hormone (GH) • Presence of tumor causes pituitary to release more GH
Hyperpituitarism • Signs and Symptoms • Dependent upon which cells of the pituitary are affected • Children • Longitudinal growth of bones, gigantism • Weight gain, failure to grow • Adult • Acromegaly = large hands, feet • Enlarged jaw, nose, lips, tongue • Thickening of facial soft tissues • Mood swings • Enlargement of internal organs (inc. heart)
Hyperpituitarism • Diabetes, hyperglycemia, hypercalcemia, hypertension, fatigue, impaired vision, headaches, arthritis
Hyperpituitarism • Treatment • Excision of adenoma or pituitary • Radiation if parts of adenoma remain • Medications to shrink tumor • Pituitary hormone replacement therapy
Physical therapy intervention For Hyperpituitarism • Muscle strengthening and management of arthritis associated with the condition may be necessary.
Graves’ Disease • Description • Hyperthyroidism = Hyperactivity of the thyroid gland with goiter • Metabolic rate can increase by 60-100% • Women > men after 20 years of age • Named after the Irish Physician Robert J. Graves, 1797 – 1853 • Etiology • Autoimmune disorder • Family predisposition may exist
Graves’ Disease • Signs and Symptoms • Hand tremors • Weight loss • Fatigue • Hypermobile joints • Unusual protrusion of the eyeballs (exophthalmos) • Reddening and swelling on the shins and tops of feet (Graves dermopathy) • Visible enlargement of the thyroid gland (goiter)
Graves’ Disease • Exophthalmos and goiter From Seidel H: Mosby’s guide to physical examination,ed 4, St. Louis, 1999, Mosby.
Graves’ Disease • Treatment • Decrease thyroid hormone production • Control signs and symptoms of the disease • Surgery to remove the thyroid • Medications – beta-blockers and antithyroidal drugs
Physical therapy intervention For Graves’ Disease • A patient with Graves’ Disease may have symptoms including muscle or soft tissue issues. The PTA must be sure not to fatigue the patient and monitor vital signs consistently. Precautions to prevent irradiation due to the patient’s contaminated saliva must be followed.
Hypothyroidism • Description • Underactive thyroid gland leading to deficiency of thyroid hormone secretion in adulthood • Cretinism, Hashimoto’s disease, congenital aplasia, secondary and tertiary • Affects 3% - 5% of population in U.S.; women > men • Etiology • Autoimmune, inherited, iodine deficiency • Thyroid is replaced by fibrous tissue -> thyroid shrinks -> reduced thyroid function
Hypothyroidism • Signs and Symptoms • Myxedema (Gull’s disease) = edema, obesity, intolerance to cold, decreased energy • Slowed metabolic rate, slowed mental processes • Muscle weakness • Thinning hair or hair loss • Treatment • Thyroid hormone medications From Seidel H: Mosby's guide to physical examination, ed 5, St. Louis, 2003, Mosby.
Physical therapy intervention For Hypothyroidism • Treatment may include strengthening and endurance activities.
Hyperparathyroidism • Description • Overproduction of parathyroid hormone (PTH) • Women > men 2:1; 100,000 in U.S. annually; increases with age • Etiology • Primary • From adenoma or hyperplasia of parathyroid -> phosphate reduction • Chronic renal insufficiency • Secondary • In response to low levels of calcium / vitamin D • Chronic renal insufficiency • Tertiary • Sharp rise in calcium levels in urine • Chronic renal insufficiency
Hyperparathyroidism • Signs and Symptoms • Hypercalcemia, hypercalciuria, high level of PTH • Renal disease • Bone resorption -> pathological fractures -> increased kyphosis and compression fractures of vertebrae • Primary • Muscle weakness, hypotonic muscles, depression, seizures • Secondary • Fractures, renal stones from calcium salt build-up, weakness, fatigue, hypertension, constipation, nausea and vomiting, mental changes
Hyperparathyroidism • Treatment • Calcimimetic medications • Nutrition supplements and dietary changes • Surgery to remove parathyroid glands
Physical therapy intervention For Hyperparathyroidism • Treatment may include gentle exercise and mobility as well as pain relief and instruction in energy conservation techniques, being careful to avoid fracture or overfatigue.
Addison’s disease • Description • Underproduction of cortisol from adrenal insufficiency • Affects females > males, usually between 30 – 50 years of age • Etiology • Failure of adrenal functions resulting from • Autoimmune disease, local or general infection, adrenal cancer, hemorrhage, sudden stoppage of medication
Addison’S disease • Signs and Symptoms • General weakness, fatigue, nausea, weight loss, diarrhea, depression, hypotension, possibly cardiac arrest • Skin coloration changes • Addisonian crisis – acute back, abdomen, or lower extremity pain, severe vomiting, diarrhea, dehydration, hypotension, loss of consciousness • Treatment • Corticosteroids or aldosterone replacement therapy
Addison’s Disease A, from Chew SL, Leslie D: Clinical endocrinology and diabetes: an illustrated colour text, Edinburgh, 2006, Churchill-Livingstone; B, from Forbes CD, Jackson WF: A color atlas and text of clinical medicine, ed 2, St. Louis, 1997, Mosby.
Physical therapy intervention For Addison’s Disease • Adrenal insufficiency may be a comorbid diagnosis for another condition for which physical therapy is indicated. Patients with Addison’s disease may where a medical alert device, and must be monitored carefully.
Cushing’s Disease / Syndrome • Description • Females aged 20 – 60 years • Excessive amounts of cortisol in the blood • Hyperpituitarism (Cushing disease) or use of corticosteroids (Cushing syndrome) • Etiology • Cushing disease • Pituitary or adrenal tumor stimulating excessive production of ACTH • Cushing syndrome • Prolonged or excessive use of high-dose cortisone drugs • Prednisone, dexamethasone, methylprednisolone
Cushing’s Disease / syndrome • Signs and Symptoms • Abdominal and facial obesity, including “moon face” and “buffalo hump”, hirsutism • Redness of face, thin skin with easy bruising, striae • Hypertension, diabetes, impaired immune system • Osteoporosis, proximal myopathy, fatigue • Treatment • Surgery to remove adrenal glands, radiation • Possible medications
Cushing’s Disease / Syndrome From Seidel H: Mosby’s guide to physical examination, ed 5, St. Louis, 2003, Mosby.
Physical therapy intervention For Cushing’s Disease / Syndrome • Treatment may be indicated for the disorders linked to Cushing’s because of the corticosteroid treatments. The PTA should be careful not to harm the skin or joints, and to guard against fractures.
Why does the PTA need to know about Diabetes mellitus? Patients with diabetes mellitus are frequently seen by PTs and PTAs for either musculoskeletal or wound care issues. It is important for the PTA to understand the precautions, contraindications, as well as the indications for the disease.
Diabetes Mellitus • Description • Lack of production of insulin by pancreas; inability of the body to utilize insulin • Type 1 diabetes: insulin dependent • Most often seen in children • Autoimmune with a genetic component • Type 2 diabetes: non-insulin dependent • Most common • Most often seen in adults, and in certain ethnic populations
Diabetes mellitus • Etiology • Type I • Destruction of islet of Langerhans beta cells following an infection or toxic exposure -> pancreas decreases little to no insulin • Idiopathic or autoimmune with genetic component • Type 2 • Resistance to insulin and altered response to glucose -> hyperglycemia • Unknown • Risk factors • African- or Asian- Americans, Pacific Islanders, Latin descent • > 45 years of age, sedentary, hypertension, high cholesterol, poor diet, obesity
Diabetes mellitus • Signs and Symptoms • Occur suddenly and more severely in Type 1; more gradually in Type 2 • Glucose in urine • Blurred vision • Weight loss, increased appetite • Nausea, vomiting, abdominal pain • Amenorrhea, erectile dysfunction • Polyuria, polydipsia, polyphagia
Diabetes Mellitus • Complications and long-term effects • Diabetic coma • Can result from both hyperglycemia and hypoglycemia • Bone disease • Osteoporosis • Cardiac and vascular diseases • Cerebrovascular disease, ischemic changes in the limb, renal disease, reflex sympathetic dystrophy, Dupuytren’s contracture, limited joint mobility, gangrene to extremities
Diabetes Mellitus • Renal disease • Reduced function to kidneys • Eye problems • Glaucoma, retinopathy, cataracts • Diabetic amyotrophy • Proximal muscle weakness • Diabetic neuropathy • Foot drop, susceptible to injury due to loss of sensation to the skin, “stocking” or “glove” parasthesias, carpel tunnel syndrome, Charcot’s joint
Diabetes Mellitus • Treatment • Insulin injections • Medications • Dietary changes • Weight loss • Regular screening of nails, feet, to minimize ulcerations • Amputation
Physical therapy intervention For Diabetes Mellitus • Exercise programs to improve blood pressure, weight loss, decrease heart rate and cholesterol levels, help body utilize insulin • Orthotic assessment, wound care for ulcers • Strengthening and lengthening of ankle musculature • Modalities to decrease pain • Rehabilitation for amputations • Pay particular attention to medication compliance
Why does the PTA need to know about Obesity? Obesity leads to other major health problems. Decreasing obesity is a focus of attention in the United States, and the PTA is able to influence his patient’s lifestyle choices such as diet and exercise.
Obesity • Description • Excess weight > WHO and CDC parameters • A goal of Healthy People 2020 is to reduce the number of overweight and obese people • Projected that >20% of U.S. population is morbidly obese • Etiology • Genetics, cultural factors • Dietary habits, diet high in fat and protein • Sedentary lifestyle • Link between adenovirus -36 and -37
Obesity • Signs and Symptoms • Relative Weight and Body Mass Index used to measure and classify • Comorbid conditions associated with obesity • Cardiovascular disease, type II diabetes, cancer • Hypertension, stroke, gallstones, osteoarthritis, sleep apnea • Treatment • Changes in diet and activity level • Medications to inhibit absorption of fat • Surgery to bypass intestine or reduce stomach size
Physical therapy intervention For Obesity • Treatment focuses on emphasizing the importance of exercising, as well as giving a high level of encouragement to the obese patient. Education regarding exercise and diet in children, adolescents, and young adults is extremely important.