Download
1 / 23
230 likes | 325 Views
Case study on accreditation: the GMC’s perspective. Martin Hart Assistant Director Education. Agenda. What GMC does How doctors are educated and trained How we accredit and quality assure Strengths of our process Issues and challenges. Our purpose.

E N D
Case study on accreditation: the GMC’s perspective Martin Hart Assistant Director Education
Agenda • What GMC does • How doctors are educated and trained • How we accredit and quality assure • Strengths of our process • Issues and challenges
Our purpose ‘to protect, promote and maintain the health and safety of the public by ensuring proper standards in the practice of medicine’
Our aim • To secure a regulatory system which: • Enhances patient safety • Fosters professionalism • Commands the confidence of all stakeholders • Is independent, fair, efficient and effective
General Medical Council A new council took office at the beginning of 2009: All appointed by the Appointments Commission
Registration Education Fitness to Practise Standards and Ethics Our functions
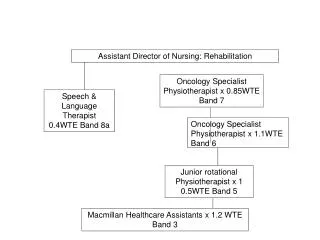
Structure of UK education and training Provisional registration Full registration Certificate of completion of training (CCT) Medical School (4-6 years) Medical School (4-6 years) F1 year (1 year) F1 year (1 year) F2 year (1 year) Specialty/ GP training (3-8 years) Specialist/GP register Career stage Employment/ regulatory status Student, not licensed Employed, licensed Employed, in training, licensed by GMC Education standards
The GMC’s role in medical education • Responsible for promoting high standards of medical education • In April 2010 PMETB will merge with the GMC • For the first time, one organisation will be responsible for regulating all stages of medical education and training
Medical School • Medical School • (4-6 years) • 32 medical schools in the UK • 35,000 medical students (60% female) • Have own approaches to curricula, teaching, assessment etc • But must all meet standards and outcomes in Tomorrow’s Doctors • Subject to fitness to practise, graduates receive provisional registration with GMC • GMC quality assures (QABME)
Foundation Programme • F1 year and F2 year • (2 years) • Foundation programme is a two year programme of general training with placements within various specialties and healthcare settings (hospital bias) • Foundation Programme has national application scheme (UKFPO) and is overseen by postgraduate deaneries • Curriculum developed by Academy of Medical Royal Colleges, approved by GMC and PMETB • F1 has outcomes set by the GMC which must be achieved to receive full registration • GMC and PMETB jointly quality assure Foundation Programme (QAFP) • 14,000 junior doctors in Foundation Programme (2009)
Specialty training • Specialty/GP training • (3-8 years) • Medical royal colleges draw up criteria for specialist and GP training and assessments, which are approved by PMETB • National competition for selection, training overseen by postgraduate deans • PMETB* certifies completion of training, leads to entry on GMC GP or specialist register and eligibility to work as a consultant • PMETB* quality assures specialist training *GMC from 2010
Maintaining Standards: Quality Assurance • Two quality assurance processes: • Foundation Programme (QAFP) • Medical Schools (QABME) • Focussed on the institution, not students and trainees • Key elements are analysis of documentation, interviews with academic staff, students and clinicians Quality assurance of specialty training currently undertaken by PMETB
Quality Assurance of Medical Education • Make sure institutions comply with standards • Identify examples of innovation and good practice • Identify concerns and help to resolve them. • Identify changes institutions need to make to comply with and a timetable for their implementation • Promote equality and diversity in medical education
QA Visit Processes QAFP • Joint process with PMETB • Postgraduate Deaneries quality management • 6 visitors • 4-day visit over 4 sites in one week • QABME • Medical Schools Quality Management • Curriculum content • Examination framework • 8 – 10 visitors • Minimum 4 days visit over 6 months • QA Reports and institutions’ replies publish on website
QA Visit Teams • Undergraduate/ postgraduate deans & school/deanery staff • Medical education specialists • Clinicians • Students/ junior doctors • Lay Visitors • All are ‘full and equal members’ of visit teams
QA visit teams • Consistent approach to recruitment • Same contracts (responsibilities, payment and time) • Mandatory annual training • Same performance management framework • Annual appraisal • Share competencies
QA Monitoring Process • Targeted action plans & updates • Annual Returns of information • PMETB Survey of Trainees (for QAFP) • Data from all three sources published on GMC website
Strengths of QABME at the end of 5 years • In depth evaluation of School • Wide range of team expertise • Interactive with School • Triangulation from multiple sources • Seen as important and generally supportive by Schools • Transparent process and status of schools’ progress on requirements is available to students and the public
Strengths of QAFP midway through • Has galvanised postgraduate deaneries to evaluate and demonstrate improvements in quality management • Has given trainees a greater voice in the quality management and assurance of their training • Has identified areas where improvements are needed particularly in the supervision of trainees • Postgraduate deaneries have reported the process as challenging and helpful – perhaps particularly the self assessment
Issues in GMC accreditation QABME & QAFP: • Resource intensive – GMC and institutions • Maintaining team focus/knowledge over cycle • Potential variability of teams • Potentially insufficient involvement of employers and patients in the QA process • Disseminating good practice/innovation
Challenges for accreditation generally • Is the QA focus on institutions sufficient for maintaining a register of professionals? • Sanctions – ‘nuclear option’: removal of accreditation • Reliance on others: can the GMC’s QA processes effectively identify areas of poor practice? • Deaneries and Schools measure the quality of individual students and junior doctors • Health systems regulator measures quality of care (and by extension doctors)
Issues for the future: Student Registration? • Medical students are not registered with the GMC • BUT guidance for schools and a significant programme of student engagement • Has the challenge of keeping in touch with students and instilling professional values been met? • Could student registration strengthen the link between the GMC and students?