Download
1 / 17
170 likes | 291 Views
Measuring the benefit of palliative chemotherapy in women with platinum refractory/ resistant ovarian cancer. Michael Friedlander Phyllis Butow, Martin Stockler, Corona Gainford, Julie Martyn, Amit Oza, Heidi Donovan, Brigitte Miller and Madeline King.

E N D
Measuring the benefit of palliative chemotherapy in women with platinum refractory/ resistant ovarian cancer Michael Friedlander Phyllis Butow, Martin Stockler, Corona Gainford, Julie Martyn, Amit Oza, Heidi Donovan, Brigitte Miller and Madeline King
Chemotherapy in platinum resistant/refractory ovarian cancer What do we know and What don’t we know? • Goal- palliation and symptom control • Objective response rates are low • Benefits as well as adverse side effects of treatment • How to best measure benefit • How does objective response correlate with symptom benefit • What % are symptomatic at the time of treatment • Do these symptoms improve
But ….still many Questions !! • Impact of treatment on HRQOL • Which instruments do we use • How important is hope in decision making? • Would good palliative care achieve the same • How much time do patients spend in hospital as a result of toxicity • How many patients receive treatment within 30 days of death • Can we identify patients most likely to benefit
Platinum Resistant Ovarian Cancer • Patients on clinical trial not necessarily representative of the population as a whole • Better Performance Status/younger etc • Objective response rates generally low -in order of 10-15% • Not clear whether symptoms improve and what price they pay for treatment
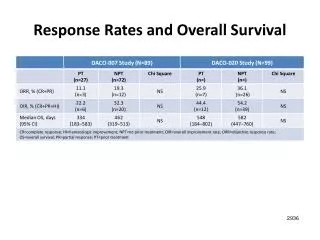
Kaplan-Meier curve of PFS ( platinum-resistant patients) Response Rates 6.5% vs. 12.3% ( NS) Median TTP- 9 vs. 13 w (NS) Median Survival 35 w vs. 41 w ( NS) 260 patients on study Gordon, A. N. et al. J Clin Oncol; 19:3312-3322 2001 Sobering reminder of the results of treatment
Response Rates Symptom Control and QOL • Response rates crude way to measure benefit • Doyle et al reported improved QOL and emotional well being in 50-60% of patients receiving 2nd line treatment while ORR was 25% • Large study using EORTC QLQ-C-30 in 500 women with recurrent ovarian cancer reported no change in QOL during treatment- i.e. no change from baseline, after 3 cycles and at completion of therapy
Chemotherapy versus hormonal treatment in patients with platinum and taxane resistant ovarian cancer- a NSGO study (NSGO-OC-0101) On behalf of NSGO G. B. Kristensen, J. Kaern, E. Åvall-Lundqvist, R. dePont Christensen, S. Grenman, M. Bergdahl, R. Sandvei, M. Baekelandt, T. Skeie-Jensen,M. Kalling, T. Hoegberg, Presented IGCS Bangkok 2008
Progression free survival Chemotherapy, median time to progression: 87 days Tamoxifen, median time to progression: 62 days HR: 0.72, 95% CI: 0.55 - 0.96, p=0.024 NSGO-OC-0101 Kristenson G 2008
Overall Quality of life scoreEORTC QOL-C30 + OV28 No significant differences between treatment groups NSGO-OC-0101 Kristenson G 2008
Possible interpretation… • 'Global QOL scale may not be sensitive enough to pick up differences' • There must be better ways to measure symptom control and palliative benefit
Makhija S et al. Proc ASCO 2007;Abstract 5507
GCIG Symptom Control Study HYPOTHESES • The subjective improvement of palliative chemotherapy and clinical benefit will be significantly greater than objective response rates. • Clinical benefit measures that incorporate both objective response and subjective improvement will provide a more meaningful method of evaluating the effect of palliative chemotherapy • It should be possible to identify which patients are more likely to benefit from palliative chemotherapy as well as the group who have little benefit i.e develop a prognostic index/score
Study Schema Target Population >18yrs platinum resistant/ refractory epithelial ovarian cancer / > 3 LINES ECOG 0-3 Able to commence treatment within 2wks of registration Sufficient English language skills to complete QoL forms independently • Stage1 • 100 patients • Complete 7 QoL • forms • 20 subjects will • participate in • additional QoL • telephone interview Data Collection 4 Treatment cycles or Disease progression REGISTER
STAGE 2 400 -500 patients Primary Objective • To determine the proportion of women benefiting from palliative chemotherapy as defined by a clinically significant improvement in HRQL scores and symptom benefit as well as objective response. Develop a better measure of symptom benefit for clinical trials Secondary Objectives • The proportion of women who receive treatment because they are (a) symptomatic, (b) have rising tumor markers alone, and or (c) have imaging evidence of disease progression alone. • The most common and important symptoms as defined by the patients themselves. • Whether these patient defined symptoms improve with chemotherapy • Whether improvements in symptoms and HRQL correlate with objective response. • The effects of treatment, objective response and subjective response on scores for anxiety, depression and hope. • Derive a prognostic index to better predict outcomes and likelihood of benefit
Conclusions- with respect to study • General: • QOL measures result in a lot of data and outcome variables to analyse & interpret • The relationship among them is complicated • Particularly so for the relationship between specific symptoms and overall QOL • Potential diluting effects with the more expansive/inclusive definitions & measures of QOL • Important to focus on the symptoms that really matter to patients in a particular context and whether they improve • In the context of palliative chemo for platinum refractory/resistant ovarian cancer: • FOSI appears to have the right content & mix for a single index measure • Likely to sensitive to palliative benefits of therapy AND to deterioration due to disease progression • We will explore all these questions in depth in our study