Download
1 / 35
350 likes | 493 Views
Integrated Chronic Model. A Foundation to Transform PCMH Care Delivery. Opportunities for Redesign. Evidence-Based Guidelines (EBG). Staff have defined roles/share responsibility for outcomes. Leadership support and vision. Health System Organization. Delivery System Design.

E N D
Integrated Chronic Model A Foundation to Transform PCMH Care Delivery
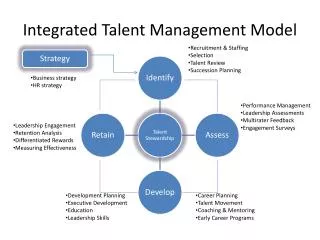
Opportunities for Redesign Evidence-Based Guidelines (EBG) Staff have defined roles/share responsibility for outcomes Leadership support and vision Health System Organization Delivery System Design Self-Management Support Decision Support Clinical InformationSystems Links to Community Resources Staff equipped with needed competencies Embed EBG/ identify high risk patients Aware of/ encourages linkages
ICM:Driving Principles Better Care, Better Health, Lower Costs
Key Components of Our High Risk Program • Population – patients meeting IHI criteria for high risk • Service delivery – in hospital if identified as appropriate, and in the community • Key interventions – Follow clinical EVG, behavioral interventions, barrier assessment and intervention planning, referrals as appropriate
Key Components of High Risk Program In hospital interventions: • Hospital-based patient assessment completed by a home health nurse liaison • Depression • Literacy level • Medication error risk • Personal assessment of risk • Ensures a medical appointment within 7 days of discharge • Initiation of red flags teaching using “teach-back” technique • Integration of care givers in discharge process/ PHR • Initiation of in-home high risk protocol
Key Components of High Risk Program Interventions provided in the home: • Nursing assessment of self-management ability, home environment, care giver support, psychosocial issues • Medication reconciliation • Ensures a medical appointment within 7 days of discharge /method of transportation/ visit preparation • Initiation/ reinforcement of red flags teaching using “teach-back” technique • Visits front loaded with first visit emphasis on care transition interventions • Self-management support and coaching to continue to engage patient/ family/ care giver • Remote monitoring
A Simple Method of Risk Stratification: Institute for Health Improvement
PHR: Identifying Gaps in Home Support
Multidisciplinary Conference • Led by Model Champion • SBAR Format • Risk assessment/ review & intervention discussion • Care plan projected along with telehealth data • Pt-centered goal emphasis
EMR Example of Decision Support -PHQ-9 Prompts Questions A-I
Patient Engagement andSelf-Management Support Patient Engagement Defined: “Actions individuals must take to obtain the greatest benefit from the health care services available to them.“ Center for Advancing Health The provision by health professionals of “self-management support” as defined by Dr. Wagner supports the activation of patients to take action. Pt Engagement SMS
Patient Engagement through the provision of Evidence-Based SMS Review of 4 Chronic Care Model (CCM) components in 39 studies – results: 19 out of 20 studies with improved outcomes included self management support (SMS). Source: Bodenheimer, et al. JAMA Oct. 2002
Engagement Implications • Engagement levels strongly correlate with satisfaction rates (78% of engaged patients rate their quality of care highly, compared with 43% of non engaged patients • Every visit offers opportunity to build or break your relationship with your patient • Hard to manage financial risk if patient doesn’t remain with the provider over time • Physicians often lack the time and tools to adequately educate and engage patients over time. • With more clinical and financial risk – partners are needed to extend the physicians influence and reach
Obstacles to Engagement • Failure to appreciate the potential impact of engagement efforts • Some clinicians still possess the “blame-the-patient” mentality • Reluctance to move away from conventional roles to one of collaboration • Using patient-facing materials that create confusion and hinder access to information and services
Getting Out of Our Comfort Zone • Where we tend to focus: • Adherence to clinical guidelines • Patient education • Directing • Where new focus is needed: • Using behavior change interventions • Building patient confidence • Guiding
Provider Competencies Needed Patient Engagement/ Therapeutic Partnerships Ability to identify/address patient barriers Expert in care coordination- facilitates effective transitions Knowledge of current evidence-based guidelines • Patient-activated • adult education and health literacy • Communication skills • & facilitation of behavior change
What is Self-Management Support? A collaborative process to help people to: • Understand • Choose among treatments • Identify and set goals • Adopt and change behaviors • Cope and overcome barriers • Follow-through
Competencies for Improving Understanding and Retention “Can you find the salt on the label? “ Patient Activated Adult Education • Identification of literacy issues • Interventions to address low literacy • Learning is relevant • Problem solving/ scenario based learning • Competent in “teach-back” technique • Patient directed learning
Goal Setting : Putting the Patient’s Priorities Front and Center Request patient answer these questions prior to face to face encounter with MD. 1. What is most important for you to accomplish during your visit? 2. What concerns you the most about your condition? 3. What specifically would you like to work on to manage your condition? • IHI Ask me 3 campaign
Ensuring Patient Choice These are some things you can do to help you with your long term goal. What would you like to work on?
Bringing the PCMH to LifeSpecific Enabling Capabilities For Consideration
Possible Physician Role • Start the conversation/ set the tone • Engage the patient/ ask about personal goals : using open ended questions & collaboration • “Warm” hand off to the team • Stay in touch/ review at each encounter
Possible Team Role • Continue to educate/no jargon • Check understanding, clarify, teach back • Identify/ resolve barriers • Collaboratively complete the action plan • Problem-solve • Plan for follow-up • Offer positive reinforcement and support – affirm in their ability to succeed 32
Considerationswhen resources are limited • Identify a small high risk sub group to maximize outcomes while minimizing resource need • Use a tightly structured process • Train MA’s/ Community volunteers in health coaching • Have Home Health function as your SMS/ DM team
We’re in this together Medicare Spending Per Beneficiary (MSPB) Quiring, C. and Thompson, S. Medicare Spending Per Beneficiary (MSPB) the New Link Between Acute and Post Acute, Remington, July/August 2012
Contact Information Paula Suter, BSN, MA, CCP Clinical Director, Integrated Care Management Sutter Care at Home suterp@sutterhealth.org