Download
1 / 79
850 likes | 1.11k Views
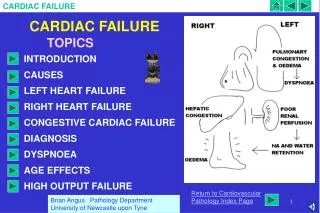
CARDIAC FAILURE. PROF H duT THERON 2010. MANAGEMENT OF HEARTFAILURE. OVERVIEW Heart failure Resulting from Compensatory mechanisms. Complex syndrome Easily recognized difficult to define. Left ventricular disfunction. systolic diastolic. Inadequate Non specific

E N D
CARDIAC FAILURE PROF H duT THERON 2010
MANAGEMENT OF HEARTFAILURE OVERVIEW • Heart failure • Resulting from • Compensatory mechanisms • Complex syndrome • Easily recognized • difficult to define • Left ventricular disfunction • systolic • diastolic • Inadequate • Non specific • Worsening cycle of events
HEALTH CARE IMPACT • 0,5 to 2% population • 200 000 to 800 000 in RSA • Adverse prognosis • Economic impact • 40% five year survival • Class 4 NYHA and IHD • 43% one year survival • 18% three year survival • Hospitalization • Reduce hospitalization • length of stay • Pharmacotherapy • ACE inhibitors - expensive • AIIRB - expensive • Loop diuretics - expensive
DEFINITION • Haemodynamic: Cardiac failure will result when the heart is unable to effectively manage the volume of blood delivered to the heart. • Pathophysiologic: Heart failure occurs when an abnormality of cardiac function causes the heart to fail to pump blood at a rate required by the metabolizing tissues or when the heart can do so only with elevased filling pressures. This inability may be due to insufficient or defective cardiac filling and or impaired contraction. • Clinical: Congestive heart failure represents a complex clinical syndrome characterized by abnormalities of LV function and neurohormonal regulation, which are accompanied by effort intolerance, fluid retention and longevity.
COMPENSATORY MECHANISMS Chamber function adaptive response PRESSURE VOLUME Figure 1: Relationship between end diastolic pressure and end diastolic volume NOTE: An increase in end diastolic volume will be accompanied by an increase in end diastolic pressure
CARDIAC OUTPUT END DIASTOLIC PRESSURE Figure 2: Starlings cardiac output curve NOTE: An increase in end diastolic pressure will lead to an increased cardiac output.
HYPER EFFECTIVE NORMAL CARDIAC OUTPUT HYPO EFFECTIVE END DIASTOLIC PRESSURE Figure 3: Guyton’s cardiac pump function curve
The 3 figures show the following • Increased end diastolic volume Almost linear related increase in end diastolic pressure • Increased end diastolic pressure ( increased end diastolic volume ) Increase in cardiac output • Starling “ Within physiological limits, the larger the volume of the heart the greater are the energy of its contraction and the amount of chemical change at each contraction.” The mechanism is effective only up to a certain point: when cardiac end diastolic volume exceeds a critical level further increases in volume will lead to a reduction in cardiac output. In the failing heart this mechanism ultimately fails to improve myocardial contractility.
VENTRICULAR REMODELLING Normal Regionally ischemic ventricle Ischemic Infarcted Normal Ischemic Infarcted After remodeling
Left ventricular dilatation • Hypertrophy may occur • Fibrosis of infarcted tissue • Cardiomegaly • Maintain stroke volume • Increase in wall stress • Increase in myocardial oxygen demand RESULT COST
REFLEX CONTROL MECHANISMS Heart failure Hypovolemia Decrease in cardiac output Reduction peripheral perfusion PERCEIVED THREAT TO CIRCULATORY HOMEOSTASIS Response Hypovolemia Reduced cardiac output • Sympathetic nervous system • Renin angiotensin • Aldosterone • Vasopressin (ADH)
THUS: The adaptive response of reduced peripheral perfusion secondary to decrease in cardiac output or hypovolemia are similar, leading to worsening cardiac failure.
ABNORMALITIES OF THE SYMPATHETIC NERVOUS SYSTEM • Cardiac output • Peripheral perfusion • Activation sympathetic nervous system • peripheral resistance • afterload • metabolic cardiac demand • cardiac output VISIOUS CYCLE OF EVENTS
RENIN ANGIOTENSIN ALDOSTERONE SYSTEM Cardiac output Peripheral perfusion Renal perfusion Angiotensinogen Renin Angiotensin CONVERTING ENZYME Angiotensin Vasoconstriction Aldosterone secretion Increase afterload Salt & water retention INCREASE CARDIAC WORKLOAD WORSENING IN CARDIAC FAILURE
VASOPRESSIN Cardiac output Baroreceptor pressure Hypothalamic blood flow Angiotensin Vasopressin Arteriolar vasoconstriction Sodium & water retention Increase afterload Volume overload Cardiac workload Cardiac output
ENDOTHELIN Endothelin levels increased Aldosterone ANF Renin
Atrial natriuretic factor (ANF) Cardiac output Volume overload Atrial dilatation ANF Aldosterone Vasodilatation Neuro endocrine activation EFFECTIVE COUNTER REGULATORY MECHANISM ANF - degradation via neutral endopeptidase Neutral endopeptidase inhibitors ANF - RX.CCF
ALDOSTERONE Cardiac output Renin angiotensin aldosterone Aldosterone levels Hypercoagulation? Na+ retention Fluid retention Myocardial fibrosis LV Hypertrophy K+ Arrythmia Vasoconstrition Afterload WORSENING CARDIAC FAILURE Important implication in pharmacological relevance for treatment of heart failure NEW
RESULT OF REFLEX CONTROL MECHANISMS • Increase vascular resistance ( afterload) • Salt & water retention ( preload) Myocardial wall stress Myocardial oxygen demand CARDIAC FAILURE BEGETS CARDIAC FAILURE
TREATMENT OF CARDIAC FAILURE Questions • Are presenting symptoms and signs related to cardiac failure • What is the ethiology • Are there precipitating factors • Evaluation needed diagnosis: systolic/diastolic • How severe is the heart failure syndrome • How should the patient be treated acutely • How should the patient be treated chronically • Medication - ? Detrimental • Life style adjustment • Surgery
PRESIPITATING FACTORS • Acute myocardial ischemia • Superimposed infections • Onset of atrial fibrillation • Alcohol abuse • Poorly controlled • Excessive dietary sodium intake • Non compliance with drug therapy • Anemia • diabetes • hypertension • hypothyroidism
ROLE OF ANEMIA ANEMIA • TACHICARDIA • INCREASE MYOCARDIAL WORL LOAD • WORSENING HEART FAILURE • ACTIVATION RAS • WORSENING HEART FAILURE CARDIAC FAILURE RENAL PERFUSION RAS ACTIVATION ERITHROPOITIN WORSENING CF ANEMIA CARDIAC FAILURE CAN PRESIPITATE ANEMIA AND ANEMIA CAN PRESIPITATE CARDIAC FAILURE THEN VISCIOUS CIRCLE OF EVENTS
CARDIAC FAILURE AS A RESULT OF SYSTOLIC DYSFUNCTION
MEDICATIONS COMMONLY USED IN HEART FAILURE TREATMENT PROTOCOLS DRUG THIAZIDE DIURETICS Hydrochlorothiazide Clorthalidone THIAZIDE RELATED AGENTS Metolazone LOOP DIURETICS Furosemide POTASSIUM-SPARING DIURETICS Spironolactone Triamterene Amiloride RECOMMENDED MAX DOSE (MG) 50 qd 50 qd 10 bid 240 bid 100 bid 100 bid 40 bid MAJOR ADVERSE REACTIONS Postural hypotension Hypokalemia,hyperglycemica, rash; rare severe reaction includes pancreatitis, bone marrow supression, and anaphylaxis Same as thiazide diuretics Same as thiazide diuretics Hyperkalemia, gynecomastia (spironolactone only)
MEDICATIONS COMMONLY USED IN HEART FAILURE TREATMENT PROTOCOLS DRUG SELECT ACE INHIBITORS Enalapril Captopril Lisinopril Quinapril ANGIOTENSIN II RECEPTOR BLOCKER Losartan Valsartan Candasartan BETA BLOCKERS DIGOXIN HYDRALAZINE ISOSORBIDE DINITRATE (Isordil) ISOSORBIDE MONONITRATE (Imdur) (Ismo) RECOMMENDED MAX DOSE (MG) 20 bid 100 mg tid 40 qd 40 qd 100 mg qd As needed 100 tid 80 tid 240 mg qd 40 mg qd MAJOR ADVERSE REACTIONS Hypotension, hyperkalemia, renal insufficiency, cough, skin rash, angioedema, neutropenia, nausea, dysgeusia Diarrhea, dyspepsia, orthostatic dizziness Cardiotoxicity, confusion, nausea, anorexia, visual disturbances Headache, nausea, dizziness, tachycardia, lupuslike syndrome Headache, hypotension, flushing Same as isosorbide dinitrate Same as isosorbide dinatrate
POSITIVE INOTROPIC AGENTS Digitalis • Controversy • Digitalis trial • Indications • Neutral effect on mortality • Reduction in hospitalization • Atrial fibrillation & CHF • Symptomatic CHF despite ACE • inhibitors & diuretics • Sinus tachycardia related CHF • Pregnancy and CHF
MILD HEART FAILURE & SINUS RHYTHM No AF or tachycardia Digoxin Not necessary
INTRAVENOUS INOTROPIC THERAPY • Adrenalin • Dobutamine • Dopamine • Milrinone • Amrinone
Diuretics • peripheral oedema • preload mycardial wall stress • myocardial oxygen demand • cardiac mechanics • cardiac output • Mainstay treatment • Relieve volume overload • Mild volume overload • Severe volume overload • Marked volume overload / pulmonary oedema • thiazide diuretic • loop diuretics • intravenous furosamide
DIRECT ACTING VASODILATORS Venodilatation Peripheral art. dilatation Preload Afterload Myocardial wall stress Impedance ventricular emptying CARDIAC WORK LOAD MYOCARDIAL OXYGEN DEMAND IMPROVE CARDIAC OUTPUT
STUDIES Isosorhide Hydralazin Conventional therapy • V Heft I • V Heft II • CONSENSUS • SOLVD • SAVE • AIRE Enalapril Hydralazin Enalapril Enalapril Captopril Acute MI Ramipril
ACE inhibitors in heart failure • Approximately 7,000 patients evaluated in placebo-controlled clinical trials • Consistent improvement in cardiac function, symptoms and clinical status • Decrease in all-cause mortality by 20-25% (p<0.001) • Decrease in combined risk of death and hospitalisation by 20-25% (p<0.001)
ANGIOTESIN CONVERTING ENZYME INHIBITORS (ACEI) Cardiac output Renal perfusion Inactive renin renin Renin substrate (angiotensinogen) Angiotensin I Angiotensin converting Enzyme ACE inhibitors Angiotensin II Pressor effect Aldosterone secretion Sympathetic stimulation Renal action
ACE INHIBITORS • Preload • Afterload • Sympathetic outflow • Aldosterone secretion Escape later Unless contra indicated or tolerated all patients with symptomatic heart failure should be treated with an ACE Inhibitor.
CONTRA INDICATIONS TO ACE TREATMENT • Cardiogenic shock • Angioneurotic oedema • Persistantly elevated potasium level • Bilateral renal artery stenosis • Pregnancy • Absolute • Relative • Hypotension - systolic BP < 90 mmHg • Impaired renal function • Hypertrophic obstructive cardiomyopathy • Tight AS or MS
ACE INHIBITORS (CONTD) Adverse events Predictable in the presence of • Hyponatremia • Orthostatic hypotension • Low BP • Renal dysfunction
ACE INHIBITORS (CONTD) General principles • Favorable effects are class related • Usually well tolerated • Avoid excessive diuresis - lower diuretics • Start low dosage • Titrate slowly upwards over weeks AIM : minimize diuretics dosage maximize ACE inhibitors dosage Alternatives : Nitrates & Hydralazine
ACE inhibitors in heart failure Consensus recommendations All patients with heart failure due to left ventricular systolic dysfunction should receive an ACE inhibitor unless they have a contraindication to its use or cannot tolerate treatment with the drug US Consensus Recommendations (1996)
ANGIOTENSIN II RECEPTOR BLOCKERS Effects = ACE inhibitors Data supports use of Losartan / Valsartan /Candesartan Indication No need to replace ACE for ARII without adequate reason Possibly no aldosterone escape ACE Inhibitor intolerance
ANGIOTENSIN II RECEPTOR BLOCKERS • ELITE 1 • LOSARTAN : CAPTOPRIL • ? REDUCTION IN MORTALITY • ELITE 2 • NO DIFFERENCE IN MORTALITY • VALHeFT • VALSARTAN : PLACEBO • MORTALITY UNAFFECTED • REDUCTION IN HOSPITALIZATION • IMPROVEMENT IN EJECTION FRACTION • CHARM • ALTERNATIVE • ADDED • PRESERVED
CHARM PROGRAMME 3 Component trials comparing candasartan to placebo in patients with symptomatic heart failure CHARM Alternative n = 2028 LVEF ≤ 40% ACE Inhibitor intolerant CHARM Preserved N = 3025 LVEF > 40% ACE Inhibitor Treated / not treated CHARM Added n = 2548 LVEF ≤ 40% ACE Inhibitor treated Primary outcome for each trial: CV death or CHF hospitalisation Primary outcome for Overall Programme: All-cause death
CHARM Programme Mortality and morbidity All Cause Mortality CV Death or CHF Hospitalisation Alternative Added Preserved Overall 0.77 P = 0.0004 0.85 P = 0.011 0.89 P = 0.118 0.91 0.84 P < 0.0001 P = 0.005 0.7 0.8 0.9 1.0 1.1 1.2 0.6 0.7 0.8 0.9 1.0 1.1 1.2 Hazard Ratio p heterogeneity = 0.37 Hazard Ratio p heterogeneity = 0.43
INDICATIONS SYSTOLIC HEART FAILURE (IMPAIRED FX ) • ACE INTOLERANCE • ? COMBINATION WITH ACE INHIBITORS • ISCHAEMIC HEART DISEASE IMPORTANT DIASTOLIC HEART FAILURE (PRESERVED FX) • NO INDICATION NO INDICATION TO REPLACE ACE INHIBITORS WITH AR BLOCKERS
CALCIUM CHANNEL ANTAGONISTS • Arteriodilators • Negative inotropic effects • Nifedepine • Diltiazim • Verapamil Amlodipine well tolerated General : Caution in their use Limited role
BETA ADRENERGIC BLOCKING AGENTS Beneficial • Decrease sympathetic outflow • Negative chronotropic effect • Negative Inotropic effect Beneficial Harmfull benefit In acute myocardial - Non ischaemic heart failure - ? • Metoprolol • Bisoprlol • Carvedelol Benefit proven Low dosages Titrate slowly CAUTION IN THEIR USE
ADRENERGIC ACTIVATION CNS sympathetic outflow Cardiac sympathetic activity Sympathetic activity to kidneys & blood vessels b1 receptors b2 receptors a1 receptors Myocyte hypertrophy & death, dilatation, ischaemia & arrhythmia's Vasoconstriction Sodium retention Packer, AHA 2000