Download
1 / 1
• 10 likes • 40 Views
Explore the advanced imaging capability of Optical Coherence Tomography (OCT) in arterial visualization, showcasing detailed vessel wall structures during balloon inflation procedures. See the feasibility study results and high-resolution imaging benefits.

E N D
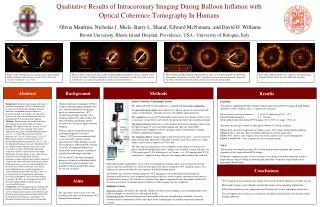
atheroma atheroma catheter I - intima signal-rich layer nearest lumen II - media signal-poor middle layer 0.53 mm 0.38 mm 2.18 mm 2.57 mm III - adventitia signal-rich outer layer balloon atheroma balloon partially inflated before balloon inflation balloon totally inflated Fig 4 A-B = Stented segment of a saphenous vein graft during balloon deflation. Struts are easily identified and sharp. Figure 1A-B. OCT imaging of a coronary artery during partial balloon inflation. Atherosclerosis results in loss of layered structures within the vessel wall. Figure 2 A-B-C. Sequence of frames collected during balloon inflation of a native coronary artery. It shows the effects of balloon angioplasty on the arterial architecture: stretch of the wall, increase in both lumen size and external diameter, and decrease in wall thickness. Background Results Abstract Methods Optical Coherence Tomography System The Light Lab OCT system hardware is comprised of four major components. An optical imaging engine emits and receives optical signals. It contains the light source, interferometer, detection circuitry and a digital signal processor. The computerprocesses OCT information and converts it for display. It also serves as an image storage device and controls the patient interface unit and optical engine. The patient interface unit serves as the interface between the imaging catheter and the optical engine. It starts and stops imaging and spins the optical fiber (circumferential imaging) inside the imaging catheter and performs automatic pullback (longitudinal imaging). The imaging catheter conducts light to the interior of the artery, receives reflected light and transmits light back to the patient interface unit. The catheter is a single lumen catheter with a diameter of 0.014-inch. The fiber-optic interferometers were coupled to a mid-infrared (1320nm), low power, broad-bandwidth light source. Images were acquired at either 8 frames /sec (250 angular pixel X 250 radial pixels) or 4 frames / sec (500 angular pixel X 250 radial pixels), displayed using a brown-scale lookup table and digitally archived. Feasibility Ten patients undergoing PCI for standard clinical indications had OCT imaging during balloon inflation: 8 native coronary artery, 5 saphaneous vein graft. Mean coronary reference diameter: 3.15 + 0.47 mm (range 2.25 - 3.27). Inflated balloon diameter: 1.5 – 2.5 mm. Mean inflation duration during OCT imaging: 46.3 + 25.9 sec (range: 15-94 sec). The above pictures give details on the high resolution (10-20µm) of images. Figure 1 a-b: describe components of coronary artery OCT image during balloon inflation Figure 2 a-b-c: show the effects of balloon inflation on arterial architecture Figure 3 b-c: show a stent segment. Structure of the arterial wall is easily distinguished Figure 3 a and 4 a-b: vessel segments just after stent placement. Optical coherence tomography (OCT) is a high-resolution imaging modality that uses advanced photonics for imaging and tissue characterization. OCT extends the principles of pulse-echo imaging employed by ultrasound to the optical domain, permitting catheter-based devices to achieve high resolution imaging. Whereas ultrasound produces images from high-frequency acoustical "echoes," OCT uses near-infrared light waves that reflect off the internal microstructure within biological tissues. The frequencies and bandwidths of light are orders of magnitude higher than medical ultrasound signals, resulting in greatly increased image resolution. The use of OCT for arterial imaging, however, is limited in that blood results in substantial signal attenuation and inability to obtain interpretable images of vascular structures. Background. Intracoronary imaging with optical coherence tomography (OCT) is limited by the presence of red blood cells. Imaging from the lumen of an expanded balloon catheter is a potential solution. Accordingly, the aim of this study was to assess the feasibility and safety of intralumenal OCT during balloon inflation. Methods. Digital images were collected using a 0.014 imaging wire in the guide wire lumen. Results. We studied 10 pts for a total of 13 OCT imaging runs (8 native coronary artery and 5 sapheneous vein graft). Inflated balloon diameter was 1.5 – 2.5 mm. Mean coronary reference diameter was 3.15 + 0.47 mm (range 2.253.27). Both stented and non-stented segments were imaged. Mean inflation duration was 46.3 + 25.9 sec. Interpretable image runs were obtained in 9/10 pts. Within stented segments, struts were easily seen and were sharp, undistorted with spatial resolution superior to intravascular ultrasound. Within non-stented segment, layers of the arterial wall were easily distinguished (intimal hyperplasia, media and adventitia) and in narrowed segments the effects of balloon inflation on arterial architecture were easily seen and quantifiable. No pts had a major adverse coronary event (death, myocardial infarction, need of urgent bypass surgery) during the procedure or after it. Also, no pt experienced any complications (dissection, occlusion or thrombosis) or an elevation of post-procedure CK. Three pts developed transient ST elevation during balloon inflation and 1 pt experienced chest pain. Conclusions. OCT imaging using an imaging wire during intracoronary balloon inflation is feasible and safe. High quality images can be obtained and provide unique arterial anatomic information. The development of ischemia as a consequence of ballonon inflation limits the duration of imaging. Computer Patient Interface Unit . Optical Engine Safety Three patients developed transient ST elevation during balloon inflation and 1 patient experienced chest pain without ECG changes. No patients experience major adverse coronary event (death, myocardial infarction, need of urgent bypass surgery) during or following the procedure. No patient experienced a post-procedure CK elevation. Imaging Catheter Protocol Following baseline angiography,an over-the-wire angioplasty balloon catheter was advanced across the target lesion. The guidewire was removed and replaced by the investigational OCT imaging catheter. The catheter was advanced within the wire lumen to the distal balloon marker. The balloon was inflated to nominal diameter. OCT imaging was initiated during balloon inflation. Automatic pull-back was then attempted and continued until the arterial segment immediately proximal to the balloon was imaged. The balloon was deflated if the patient experienced chest discomfort, marked ST-elevation or evidence of hemodynamic instability or if the imaging run was completed. Eligibility Criteria Inclusion criteria: technically and clinically suitable for intravascular imaging; successful placement of the balloon angioplasty catheter across the targeted lesion. Exclusion criteria: catheterization for acute myocardial infarction; hemodynamic instability; extensive coronary disease immediately distal to the target lesion; unwillingness or inability to provide informed consent. Conclusions Aims OCT imaging using an imaging wire during intracoronary balloon inflation is feasible and safe. High quality images can be obtained and provide unique arterial anatomic information. Full balloon inflation create compression and distortion of vascular and plaque architecture. The development of ischemia as a consequence of balloon inflation limits the duration of this imaging approach. The aim of this study was to assess the feasibility and safety of intralumenal OCT during balloon inflation. Qualitative Results of Intracoronary Imaging During Balloon Inflation with Optical Coherence Tomography In HumansOlivia Manfrini, Nicholas J. Miele, Barry L. Sharaf, Edward McNamara, and David O. Williams Brown University, Rhode Island Hospital, Providence, USA - University of Bologna, Italy Fig 3 Automatic pullback during balloon inflation. Fig 3 A. A stented segment. On the bottom: longitudinal view of the vessel. Fig 3 B-C: show the vessel in a non-stent proximal segment. In the absence of atherosclerosis the layers of the artery are easily distinguished.