Download
1 / 51

E N D
Case study • A two-week-old neonate is brought to your clinic by his mother who explains that her child is wheezing. Upon examination, you note an afebrile infant with a wheeze, stacatto cough, and increased anterior-posterior diameter of the chest. The lungs are tympanitic to percussion and the eyes appear crusty bilaterally.
INTRODUCTION • CHLAMYDIAE: Obligate intracellular bacteria • Family- CHLAMYDIACEAE • Classification of Family Chlamydiaceae (2 genera)
3 species causing human disease: • C.trachomatis • C.psittaci • C.pneumoniae
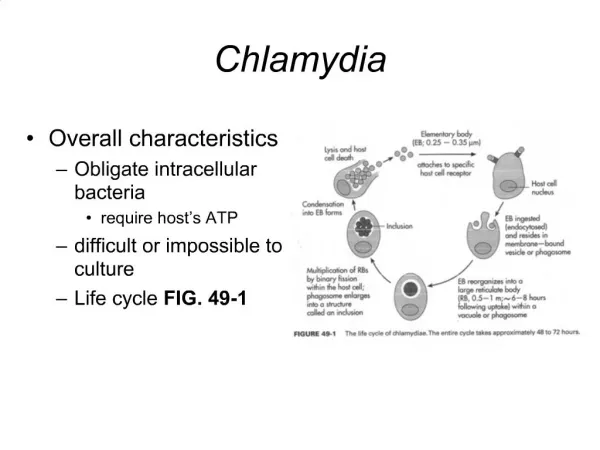
FEATURES • Small obligate intra cellular Gram negative bacteria: poorly stained by Gram’s stain • Possess RNA, DNA, ribosomes, cell wall similar to GNB • Absence of peptidoglycan is the only difference • They lack ability to generate their own ATP. So use host ATP. • Divide, multiply by binary fission
Readily stained by GIEMSA, CASTANEDA • Castaneda - blue colour -
Demonstrated by direct immuno-fluorescence They multiply in the cytoplasm of the host cell forming micro colonies or inclusion bodies which drape around the nucleus like a cloak- “Chlamys” means mantle.
Antigenic structure: Chlamydiae possess the following antigens: • Genus specific Ag: Lipopolysaccharide (LPS): Imp in pathogenesis by induction of TNF-α: leading to scarring and fibrosis. • Species specific protein Ag: • Serovar specific Ags: Major Outer Membrane Protein (MOMP) used in micro-immunoflourescence
They infect wide spectrum of vertebrate hosts- birds, mammals and humans. • Susceptible to wide range of antibiotics- tetracycline, erythromycin, macrolides, rifampicin. • C.trachomatis also sensitive to sulfonamides whereas C.psittaci and C.pneumoniae are resistant
DEVELOPMENT / LIFE CYCLE • Chlamydiae exist in 2 distinct forms- 1. EB- Elementary Body 2. RB- Reticulate Body
ELEMENTARY BODY(EB): • Extra-cellular infectious particle • Small (250-350nm diameter) • Spherical in case of C.trachomatis and C.psittaci. Pear shaped in C.pneumoniae • Has irregular electron dense nucleoli • Capable of extra cellular survival
RETICULATE BODIES(RB)- 1. Intra cellular 2. Metabolically active 3. Divides by binary fision to form EBs. 4. 800-1200nm in diameter 5. Cell wall lacks disulfide cross linking
ATTACHEMENT: • Infection is initiated by the attachment of infectious EB to susceptible host cells Eg: Biovars- Trachoma- Squamous, columnar cell C.trachomatis- LGV- lymphoid cell C.psittaci- wide range of cells INTRACELLULAR SURVIVAL: Organism enters host cell within a vesicle. Chlamydiae dependant modification of endocyte membrane prevents the lysosomal fusion and thus prevent degradation.
Conversion of EB to RB: 9 hours after infection - EB within the vesicle loses its dense DNA core, cell wall becomes less rigid due to breaking of disulfide bonds, increases in size and differentiates into RB. • 18 hours after infection- the vesicle is enlarged, RB divides by binary fission, yields pleomorphic organisms and genus specific chlamydial antigens become associated with the host cell surface.
Formation of chlamydial micro colonies within the vesicle is termed an INCLUSION BODY (IB). • It is typically peri-nuclear and may have 100-500 EBs. • By 40-70 hrs: Infectious EBs are released from the cell by rupture and these may infect new cells.
CHLAMYDIA TRACHOMATIS: • Human pathogen causing: ocular, genital & neonatal infections • C.trachomatis possess 3 biovars, • Causing trachoma & inclusion conjunctivitis (TRIC) • Those causing LGV • Urethritis, PID & neonatal infection
Based on antigenic structure of MOMP 18 serovars of C.trachomatis are identified;
PathogeniCity– Chlamydiae produce infection of eye, male and female genital tract infection and respiratory tract infections.
C.trachomatisserovars A, B, Ba & C • Trachoma– Communicable chronic kerato-conjunctivitis • Transmitted through direct contact with eye discharge from infected patients (fingers, flies fomites) • Common in young children • Acute infection: Follicles, papillary hyperplasia, pannus formation and in late stages cicatrization, blindness. • Causes blindness in trachoma belt – North Africa to South east Asia, Middle east, North India
Inclusion – conjunctivitis- C.trachomatis biovar TRIC serovars D-K. • Natural habitat: genital tract of both sexes. • Sexually active young people, spread from genitalia to eye. • Onset is acute, intense hyperemia, muco purulent discharge & follicular hyperplasia. • Unlike trachoma, this is most pronounced in the lower eye lid.
3. Opthalmia neonatrum[Inclusion blenorrhoea] • Neonatal form of inclusion conjunctivitis. • Infection acquired through birth canal. • 5-12% pregnant woman have chlamydial infection of cervix, 50% infants born to such mothers will have conjunctivitis. • 5-12 days after birth – neonate has swelling of eye lids, hyperemia and a purulent infiltration of conjunctiva. • A proportion of untreated neonates develop pneumonia.
Genital infections: • Serovar D-K – cause 30% cases of NGU • Other organisms of NGU are – Ureaplasmaurealyticum, Mycoplasma genitalium, M.hominis, Bacteroides urealyticus, CMV, T.vaginalis. • C.trachomatis also responsible for 50% cases of epidydimitis in men under 35 years of age and 15% men above 35 years.
Females – C.trachomatis serovars D-K cause urethritis mucopurulent cervicitis, vaginitis and vaginal discharge, endometritis, salphingitis, infertility, perihepatitis and periappendicitis • Endometritis and salphingitis singly or together is called PID
After 1-2 months – regional lymph node [inguinal in male and intrapelvic and pararectal in females] become enlarged and tender and may break open with sinuses. These enlarged lymph node are called BUBOS.
Respiratory tract infection: • TW 183 and AR 39 isolated in 1965 from eye of child with trachoma in Taiwan. Same strains also isolated from pharyngitis • These two organism were called TWAR. • But now classified as C.pneumonia. • It appears as the third most common cause of pneumonia after S. pneumoniae & H.influenzae.
Chlamydophila psittaci: • It also causes acute lower respiratory infection in man. • Psittacosis is disease of birds belonging to psittacine family-parrots, transmissible to man (Zoonotic disease).
Infection in birds exists as asymptomatic, latent infection which can flare up following stress to birds like caging, overcrowding.
Fecal discharge and nasal discharge of these birds will contain many organisms: source of infection to other birds and humans. • Man gets infection by inhalation of dried feces of birds. • Incubation period 1-2 weeks.
Clinical disease – mild influenza like syndrome. – fever, general malaise, anorexia, rigors, sore throat and photophobia. • Severe disease: pneumonia, septicemia, meningo-encephalitis, pericarditis, myocarditis, endocarditis, arthritis or a typhoid like syndrome having enlarged liver, spleen and a rash.
Laboratory diagnosis: • Collection of specimens – Ocular, urethral, vaginal, cervical specimen are best collected by scraping the mucosa. • Depending on the site of involvement: blood, respiratory secretions, sputum can be collected. • In LGV pus from bubo to be collected.
Processing of specimen- Direct detection of chlamydial antigens. • Light microscopy: infection of conjunctiva, urethra can be diagnosed – demonstration of typical inclusion bodies surrounding the nucleus [HP bodies] • Stain by Giemsa, Castaneda or Macchiaevello methods. • Glycogen matrix in C.trachomatis – Iodine staining – but weak or low sensitivity.
b. Immunofluorescence: FITC labeled mAb against species specific or genus specific Ag of C.trachomatis is used. • -Genus specific, also detect C.psittaci, C.pneumoniae. • -Sensitivity and specificity 90% and 95%. • -It is rapid method done under 1 hour.
2. ELISA for chlamydial antigens : Detection of soluble genus specific antigen captured by antibody attached to a solid surface eg. Plastic bead or micortiter well and later detected with enzyme labeled detector system and chromogenic substrate. • Sensitivity and specificity similar to IF.
3. DNA probes/ NAAT: DNA hybridization can be used for direct detection of C.trachomatis antigen in conjunctival and cervical smears. • PCR – Polymerase Chain Reaction – common endogenus plasmid DNA, the ompl gene [codes for MOMP] and the 16s rRNA gene can be amplified and detected by PCR. • This method is more sensitive than culture.
4. Chemilumnescence assay – • acridium – ester labeled ss DNA probe which is complementary to RNA of C.trachomatis is used. • The labeled DNA, RNA hybrid is detected in a luminometer. • Luminometer measures the light emitted by the acridium ester label. • Sensitivity and specificity 95%.
5. CULTURAL CHARACTERS: Imp. for laboratory diagnosis. Obligate intracellular paratsite: Cultivated inside: • Yolk sac of chick embryo • Cell cultures • Animal inoculation: Intranasal, intraperitoneal, intraurethral inoculation into mice.
Mice will die within 10 days. Smears taken from lung, peritoneal exudates, spleen or brain show EBS. b. Yolk sac – organism here multiply in the endothelial cells. Detected by making impression smears – Stained by Giemsa, Machivello, Gimenez, C. trachomatis grow at 35oC, C.psittaci at 39oC
c. Cell culture – Cells have to be irradiated or treated with metabolic inhibitor for isolation. Cycloheximide treated McCoy cells most commonly used. C.pneumoniae grow better in HeLa cells or Monkey Kidney cell lines. • Mouse fibroblast cells can also be used. • C. psittaci can be propagated in fish or lizard cells. • Presence of organism – detected by staining for inclusions or EBs by IF or Giemsa.
Role of Serology: Detection of chlamydialAb: Ab against C.psittaci and serovars L1 – L3 of C.trachomatis can be detected by CF test. • Ab against C.trachomatis and C.pneumoniae can be detected by micro immunofluorescence using EB’s of standard serovars. Also can use immunoperoxidase and ELISA test. • High level of IgM [>1:64] and rising titer of IgG diagnostic.
Treatment • Trachoma – Azithromycin DOC, Erythromycin & Doxycycline • Genital infections & Inclusion conjunctivitis: Doxycycline & Azithromycin • LGV : Doxycycline & Sulfonamides • Respiratory tract infections: tetracycline or erythromycin