Download
1 / 35
350 likes | 856 Views
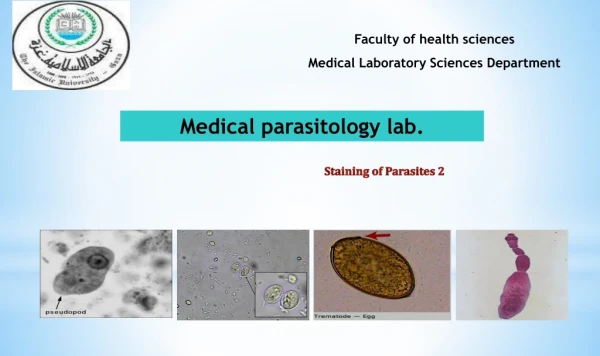
Faculty of health sciences Medical Laboratory Sciences Department. Medical parasitology lab. Thick & Thin Blood Smear. Blood Examination. The most commonly used technique for blood examination is stained blood films. Geimsa stain is usually used to stain the films.

E N D
Faculty of health sciences Medical Laboratory Sciences Department Medical parasitology lab. Thick & Thin Blood Smear
Blood Examination • The most commonly used technique for blood examination is stained blood films. • Geimsa stain is usually used to stain the films. • Delafild’shaematoxylin stain is used for microfilariae. • Either thick or thin films may be used depending on the circumstances. • The thick filmis more sensitive in detecting parasite and also saves time in examination. • The thin filmtechnique cause very little distortion of the parasite, and permits species identification when it may not be possible in thick films, but many fields must be examined to detect parasite when they are few in number.
Continue ……… • Therefore, both thick and thin films must always be prepared when searching for plasmodia and trypanosomes. • If a precise identification can not be made from thick film, the thin film will be available. • Thick films should be used when searching for microfilariae. • The most economical use of slides is achieved by making a combination thick and thin slide. • However, combination films must dry thoroughly 8-10 hrs. to overnight before they can be satisfactorily stained. • Slides for malaria should be stained in the same day.
Continue ……… • The thin films will dry quickly and can be stained as soon as they are dry, and examine for parasites. • If parasites are not seen in the thin film, stain the thick film using Field’s stain, and examine for parasites. • Direct wet mounts of fresh whole blood (or centrifuged blood) are usually used for detection of microfilariae and trypanosomes, this only gives evidence of infection and stained films are necessary for confirmation of species present. • In areas where malaria, trypanosomes, and/or microfilariae may all present, both wet and stained films should be prepared and examined. • If neither trypanosomes nor microfilariae occur in region, only stained smears need to be made for detection of plasmodia.
Examination of Thick & Thin blood smear • For optimum staining, the thick and thin films should be made on separate slides and different concentrations used for staining. • When it’s done good quality staining of thick film is of primary importance, best results are obtained if the blood smear have dried overnight. • Fixation of thin blood film done by adding 3 drops of methanol, or dipping it in a container of methanol for few seconds, with prolonged fixation it may be difficult to demonstrate Schuffner’s dots and Maurer’s dots. • To permit dehemoglobinization, thick film should not be fixed; therefore avoid exposure to methanol or methanol vapor
Reading of Thick Film • Focus on film with 10x objective and search for microfilariae. They are easily detected with 10x objective. • If microfilariae are present, switch to oil- immersion objective and identify the species. • Also, look for malaria parasites with oil- immersion objective, at least 100 fields should be examined. • Microscopy of thick film should reveal the following features: • The background should be clean, free from debris, with a pale mottled- gray color derived from the lysed erythrocytes. • Leukocyte nuclei are stained a deep, rich purple. • Malaria parasite are well defined with deep- red chromatin and pale purplish blue cytoplasm.
Reading of Thin Film • Focus with the 10x objective on the thin terminal end of the film where the RBCs are in one layer, put oil drop on the slide and switch to the oil-immersion objective. • When examining fro malaria parasites and trypanosomes, at least 200 fields should be examined. • Microscopy of thin film should reveal the following features: • The background should be clean and free from debris; erythrocytes are stained a pale greyish pink. • Neutrophil leukocytes have deep purple nuclei and well defined granules. • Malaria parasite are well defined with deep- red chromatin and pale purplish blue cytoplasm. • Like plasmodia, the cytoplasm of trypanosomes stain blue, the nucleus and kinetoplast stain red or purple.
Identification of malarial parasites • In thin films, look at the appearance of the parasite and the appearance of the RBCs containing the parasites. • The appearance of the parasites • The appearance of the RBC containing the parasites: • Size & Shape: Is the parasitized cell the same size as the blood cell without parasite or Is it enlarged? • Stippling: Is the RBC filled with pink or red staining dots? • Schuffner’s stippling in the “ghost” of the erythrocyte can some times be seen at the edges of the film and indicate infection with Plasmodium vivaxor P. ovale,. • Maurer’s dots show as stippling in erythrocytes containing the larger ring forms of Plasmodium falciparum.
Blood Parasites Trypanosoma spp.
Trypanosoma spp. • Trypanosoma cruzi(Americans) cause Chaga’s disease. • Trypanosoma bruzi(Africans) cause sleeping sickness disease. • Trypanosoma have many stages: • Amastigote, Promastigote, Epimastigote and Trypomastigote. • Reservoir host: mammalian animal. • Intermediate host: • Tsetsefly (Glossina spp.) for Trypanosoma bruzi • Reduviidae bug for Trypanosoma cruzi • Definitive host: Human. • Infective stage: Metacyclictrypomastigote. • Diagnostic stage: Trypomastigote.
Continue …… • Diagnosis: • Detection of Trypanosoma chancer after bite • Blood smear within 21 days from the bite, it will show the parasites. • Lymph node aspiration (most reliable). • Lumber puncture if brain affected. Undulating membrane kinetoblast Nucleus Flagellum
Blood Parasites Leishmania spp.
Leishmania spp. • There is many species affect man: • Leishmania tropica: cause skin lesion ( cutaneous ) • Leishmaniabraziliense: cause muco-cutaneous lesion. • Leishmaniadonovani : cause visceral lesion. • Leishmania have two stages: • Amastigote (Leishmania stage), in man (reticuloendothelial cell). • Promastigote (Leptomonas stage), the infective stage and present in the lumen gut of the sand fly. • Reservoir host: dogs and rodents. • Intermediate host: Sand fly (Phlebotomus). • Definitive host: Human.
Continue …… • Diagnosis: • Thick and thin blood film • Skin scraping • Blood culture on N.N.N media* • Serological tests Nucleus Flagellum
Blood Parasites Plasmodium spp.
Plasmodium spp. • Four species of Plasmodium are the causative agent of malaria, these are: • P. vivax, P. malariae, P. falciparum, and P. ovale. • Intermediate host: Human. • Definitive host: Anopheles mosquitoes. • Plasmodium spp. have 4 stages: • Ring form (young trophozoite.) • Late ( old ) trophozoite • Schizonts • Gametocyte. • Infective stage: Sporozoites. • Diagnosis: • Thick and stained thin blood film to detect parasites.
Ring form P. ovale P. vivax P. falciparum P. malariae
Trophozoite form P. ovale P. vivax P. falciparum P. malariae
Schizonts form P. ovale P. vivax P. falciparum P. malariae
Gametocyte form P. ovale P. vivax P. falciparum P. malariae